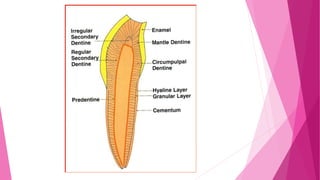
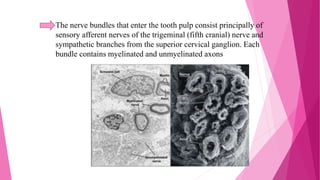
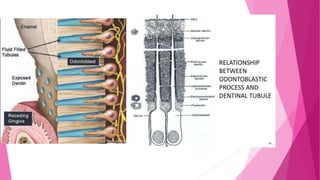
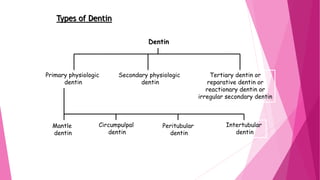
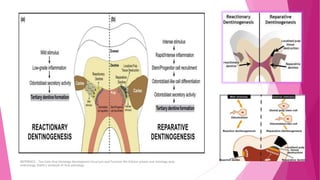
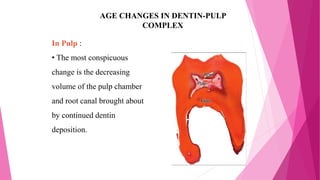
The document discusses the pulp-dentin complex. It describes dentin as the second layer of the tooth that provides structure and determines tooth shape. Dentin is a living tissue containing odontoblast processes in tubules. Dentin forms through secretion of an organic matrix followed by mineralization. Different types of dentin form throughout life. The pulp contains blood vessels, nerves and odontoblasts that form dentin. Dentin-pulp complex has sensory and protective functions.