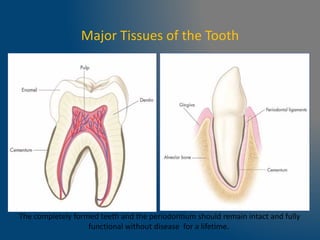
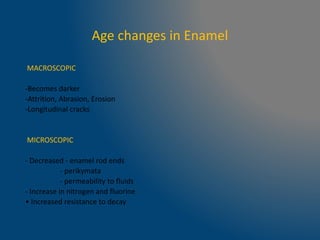
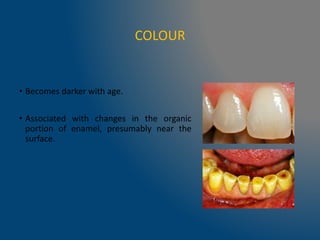
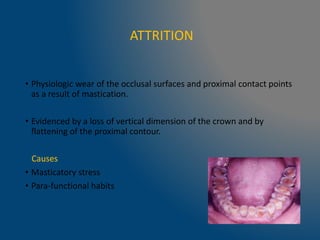
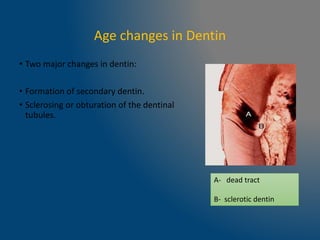
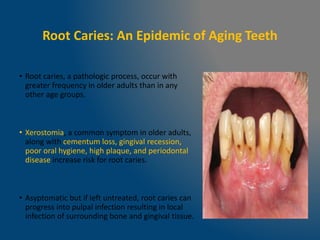
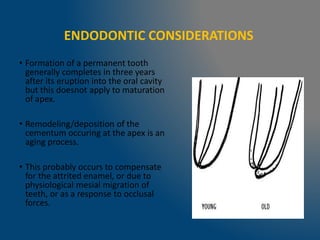
The document details the age-related changes in human teeth, including alterations in enamel, dentin, and pulp, highlighting the processes of attrition, abrasion, erosion, and the formation of secondary dentin. With age, teeth become darker and more brittle, dentinal tubules may occlude, and pulp volume decreases, leading to reduced sensitivity and reparative capabilities. Additionally, conditions like root caries are noted to be more prevalent in older adults due to factors such as xerostomia and dental hygiene challenges.
































![Age changes in enamel, dentin and pulp1 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/agechangesinenameldentinandpulp1autosaved-240807163606-82ece9c9-thumbnail.jpg?width=640&height=640&fit=bounds)
















































