The document discusses dental plaque and disclosing agents, defining plaque as a microbial biofilm that plays a significant role in periodontal disease development. It describes the history, utility, ideal properties, and various dye compositions used in disclosing agents that enhance patient motivation and effectiveness of oral hygiene practices. Methods of application for these agents are also covered, emphasizing their role in plaque identification and education for better oral health.

![ The use of agents which stain and disclose bacterial plaque in situ is
generally thought to enhance motivation by enabling the patient to detect
deposits on the teeth and to control the efficacy of his oral hygiene
techniques.
Home care aids: 1. Tooth brushing methods
2. Dentifrices(ShoPlaq , PlaqueHD)
may contain plaque disclosing agent that permits dental plaque
observation.
Staining of bacterial plaque aids in efficient plaque removal teaches the
significance of plaque in periodontal disease.
Shefali Sharma 2010. Plaque Disclosing Agent – A Review. J Adv Dental Research.2[1]:1-3 10](https://image.slidesharecdn.com/disclosingagents-copy-170420212725/85/PLAQUE-DISCLOSING-AGENTS-10-320.jpg)
![Raybin (1943):
A disclosing agent is a solution which when applied on the tooth,
makes visible by staining roughness and foreign matter on the tooth.
World English Dictionary:
A disclosing agent is a dye in liquid or tablet form that colors
something, especially the teeth to show plaque.
V. DEFINITION OF DISCLOSING AGENT
11Shefali Sharma 2010. Plaque Disclosing Agent – A Review. J Adv Dental Research.2[1]:1-3](https://image.slidesharecdn.com/disclosingagents-copy-170420212725/85/PLAQUE-DISCLOSING-AGENTS-11-320.jpg)
![VI. HISTORY
1. Skinner in 1914: First disclosing solution (Skinner’s
iodine solution). Patients' teeth were disclosed with this
solution to demonstrate "soft accumulations" which
had to be removed by the patient at home.
2. Berwick in 1920: Combination of Brilliant green –
crystal violet.
3. Easlick in 1935: Bismark brown.
4. Raybin in 1943: Gentian violet (non-iodine dye)e
Cohen et al 1972. A Comparison of Bacterial Plaque Disclosants in Periodontal
Disease. J Periodonol.43[6]: 333-338. 12](https://image.slidesharecdn.com/disclosingagents-copy-170420212725/85/PLAQUE-DISCLOSING-AGENTS-12-320.jpg)
![VII. UTILITY OF DISCLOSING AGENT
a. Diagnosing the dental plaque.
b. Personalized patient instruction and motivation.
c. Self- evaluation by the patient.
d. To evaluate the effectiveness of oral hygiene maintenance.
e. Preparation of plaque indices.
13Shefali Sharma 2010. Plaque Disclosing Agent – A Review. J Adv Dental Research.2[1]:1-3](https://image.slidesharecdn.com/disclosingagents-copy-170420212725/85/PLAQUE-DISCLOSING-AGENTS-13-320.jpg)
![1. Taste:
i. Patient comfort.
ii. Flavored.
iii. Should encourage patient co-operation.
2. Intensity of color:
i. Evident contrast to differentiate from surrounding environment.
3. Duration of Intensity: Retentive – The color should not rinse off with
ordinary rinsing methods for the period of time required to complete the
instructions or clinical examination.
4. Non-irritating to oral mucosa.
5. Non-allergic.
6. Antiseptic property.
VIII. IDEAL PROPERTIES
14Shefali Sharma 2010. Plaque Disclosing Agent – A Review. J Adv Dental Research.2[1]:1-3](https://image.slidesharecdn.com/disclosingagents-copy-170420212725/85/PLAQUE-DISCLOSING-AGENTS-14-320.jpg)
![i. Disclosing agents work by changing the color of dental plaque so
that it contrasts with the white tooth surface.
ii. Dental plaque has the ability to retain a large number of dye
substances which can be used for disclosing purposes. This
property is related to interaction, because of the polarity difference
between the components of plaque and dyes(Gallagher et al, 1977).
The particles are bound to the surface by electrostatic
interaction(proteins) and hydrogen bonds(polysaccharides).
Chetrus and Ion 2013. Dental Plaque – classification, formation, and identification.
International Journal of Medical Dentistry.3[2]:139-143.
17
X. MECHANISM OF ACTION](https://image.slidesharecdn.com/disclosingagents-copy-170420212725/85/PLAQUE-DISCLOSING-AGENTS-17-320.jpg)
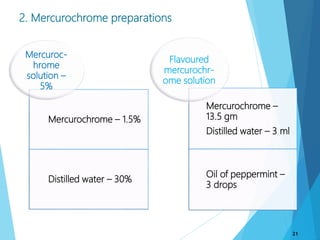
![2. Mercurochrome
preparations
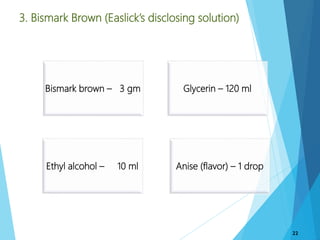
3. Bismark brown
1. Iodine
preparations
5. Erythrosin
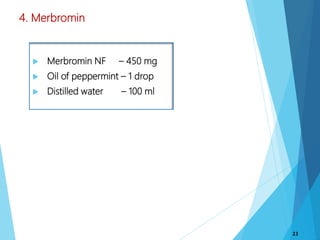
4. Merbromin
6. Fast green
8. Two tone
solution
9. Basic fuchsin
10. Three tone gel
7. Fluorescein
XI. DYES USED AS DISCLOSING AGENTS
18Shefali Sharma 2010. Plaque Disclosing Agent – A Review. J Adv Dental Research.2[1]:1-3](https://image.slidesharecdn.com/disclosingagents-copy-170420212725/85/PLAQUE-DISCLOSING-AGENTS-18-320.jpg)








![XV. REFERENCES
1. Newman et al. Carranza’s Clinical Periodontology. ed.3. W.B. Saunders Co.2002.
2. Dumitrescu AL. Etiology and Pathogenesis of Periodontal disease: Springer – Verlag
Berlin Heidelberg, 2010.
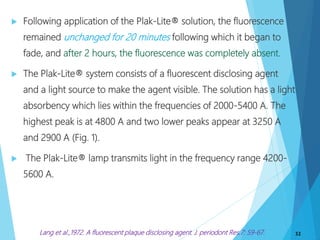
3. Lang et al 1972. A fluorescent plaque disclosing agent. J. Periodont.Res. 7: 59-67.
4. Shefali Sharma 2010. Plaque Disclosing Agent – A Review. J Adv Dental
Research.2[1]:1-3
5. Cohen et al 1972. A Comparison of Bacterial Plaque Disclosants in Periodontal
Disease. J Periodonol.43[6]: 333-338.
6. Skaggs et al.,1991. Plaque Disclosing Compositions. United States Patent: 1-7.
7. Chetrus and Ion 2013. Dental Plaque – classification, formation, and identification.
International Journal of Medical Dentistry.3[2]:139-143.
8. Block et al 1973. Dental Plaque Disclosing Agent. United States Patent:1-6.
9. Lang et al.,1972. A fluorescent plaque disclosing agent. J. periodont Res.7: 59-67.
10. Montevecchi et al.2012. The use of a Disclosing Agent During Resective Periodontal
Surgery for Improved Removal of Biofilm. The Open Dentistry Journal(6):46-50.
54](https://image.slidesharecdn.com/disclosingagents-copy-170420212725/85/PLAQUE-DISCLOSING-AGENTS-54-320.jpg)




































































