Downloaded 139 times


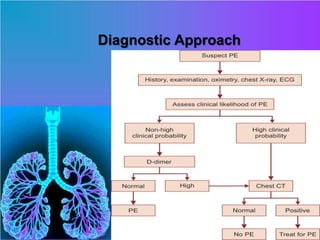



1) Pulmonary embolism is a blockage in the pulmonary artery or its branches by a blood clot that originated in the veins, causing serious health risks. 2) Risk factors include prolonged bed rest, cancer, smoking, oral contraceptive use, and pregnancy. Symptoms include dyspnea, chest pain, cough, and leg pain. Diagnosis involves tests like CT pulmonary angiography and ventilation-perfusion scanning. 3) Treatment involves oxygen, anticoagulant drugs like heparin and warfarin, and sometimes surgical embolectomy for severe cases. Prevention focuses on leg exercises, early ambulation, and compression stockings.












































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









