Downloaded 138 times


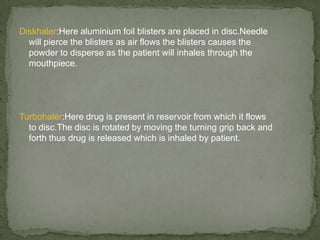
![1.Difficulty in using aerosol devices.
2.Low reproducibility of devices which is unacceptable in cases of
drugs with therapeutic index.
3.Absorption limited by the mucous layer.
4.Mucociliary clearance reduces the retention of drugs in the lungs
[this is not good in poorly soluble or slow absorbed]](https://image.slidesharecdn.com/pulmonary-121015103321-phpapp02/85/Pulmonary-5-320.jpg)



This document summarizes pulmonary drug delivery systems. It discusses the advantages of pulmonary delivery including rapid drug absorption and avoidance of first-pass metabolism. It also discusses disadvantages like difficulty using inhaler devices and mucociliary clearance reducing drug retention. Factors affecting particle distribution in the lungs like inspiratory flow rate and particle size are also covered. Finally, it describes various pulmonary delivery devices including metered dose inhalers, dry powder inhalers, and nebulizers.















































































