Downloaded 370 times
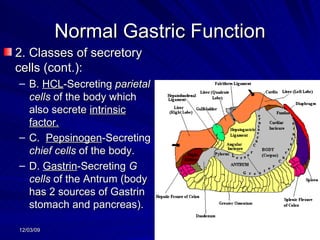
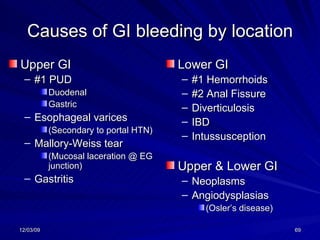


A 55-year-old male presented with epigastric pain for one month that was relieved by food but worsened 1-3 hours later. He also reported fatigue, dyspepsia, bloating, and weight loss. Differential diagnoses included peptic ulcer disease, pancreatitis, and gallstones. Recommended tests included a CBC, chemistries, H. pylori testing, EKG, CXR, and possible endoscopy or barium study. Treatment options included antacids, H2 blockers, PPIs, and antibiotics.























![Hepatomegaly[1]](https://cdn.slidesharecdn.com/ss_thumbnails/hepatomegaly1-140726111452-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)











