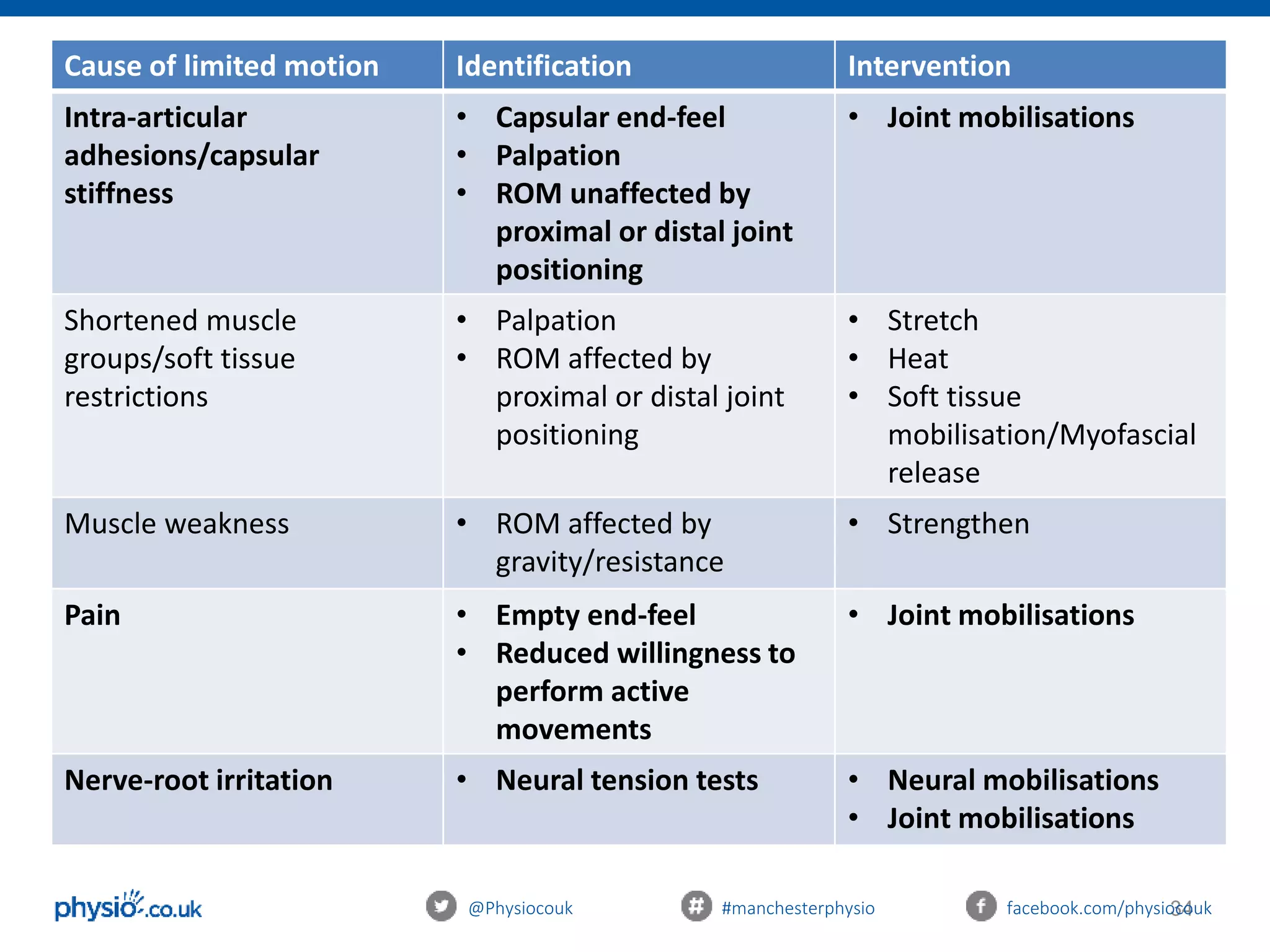
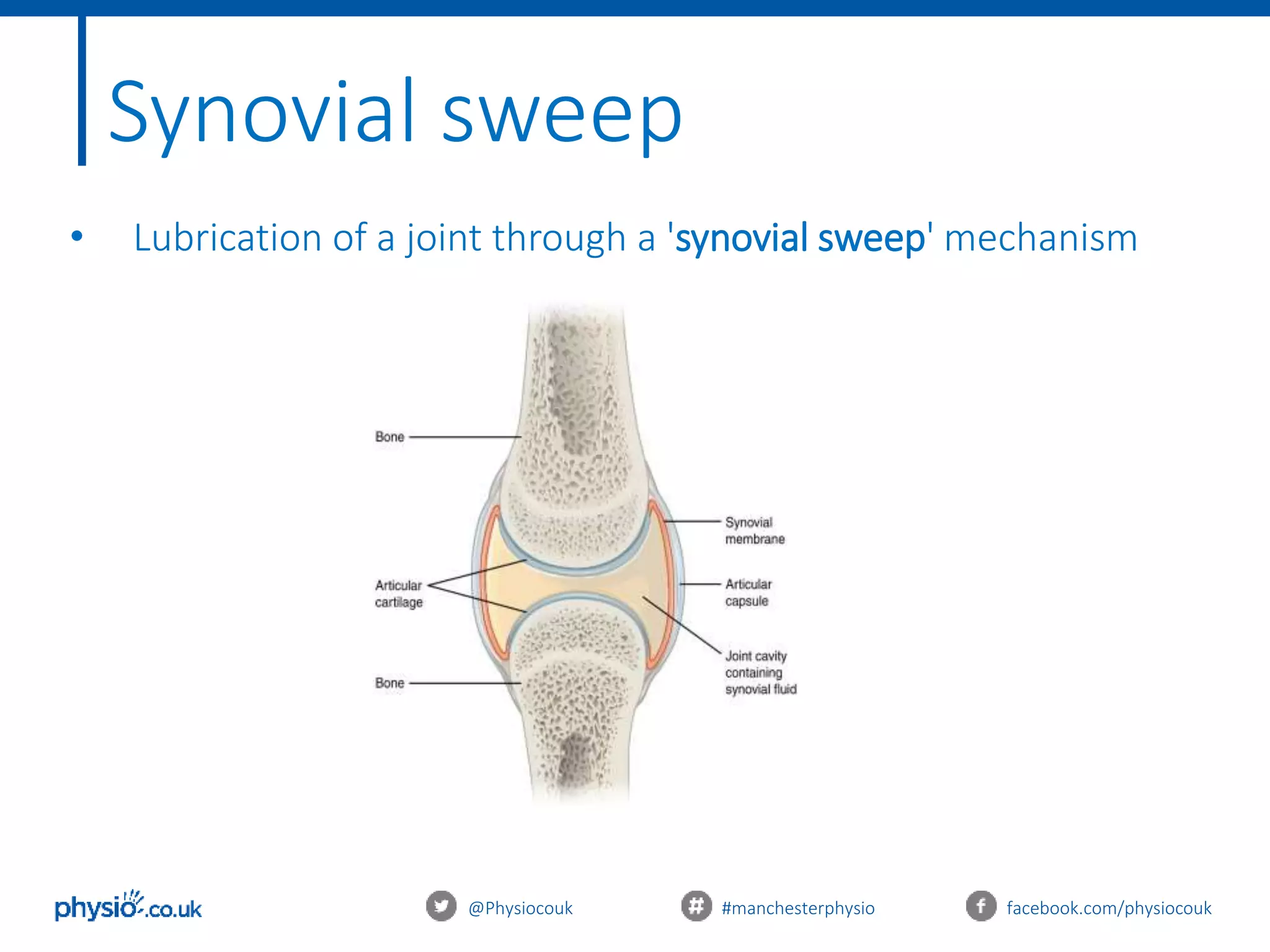
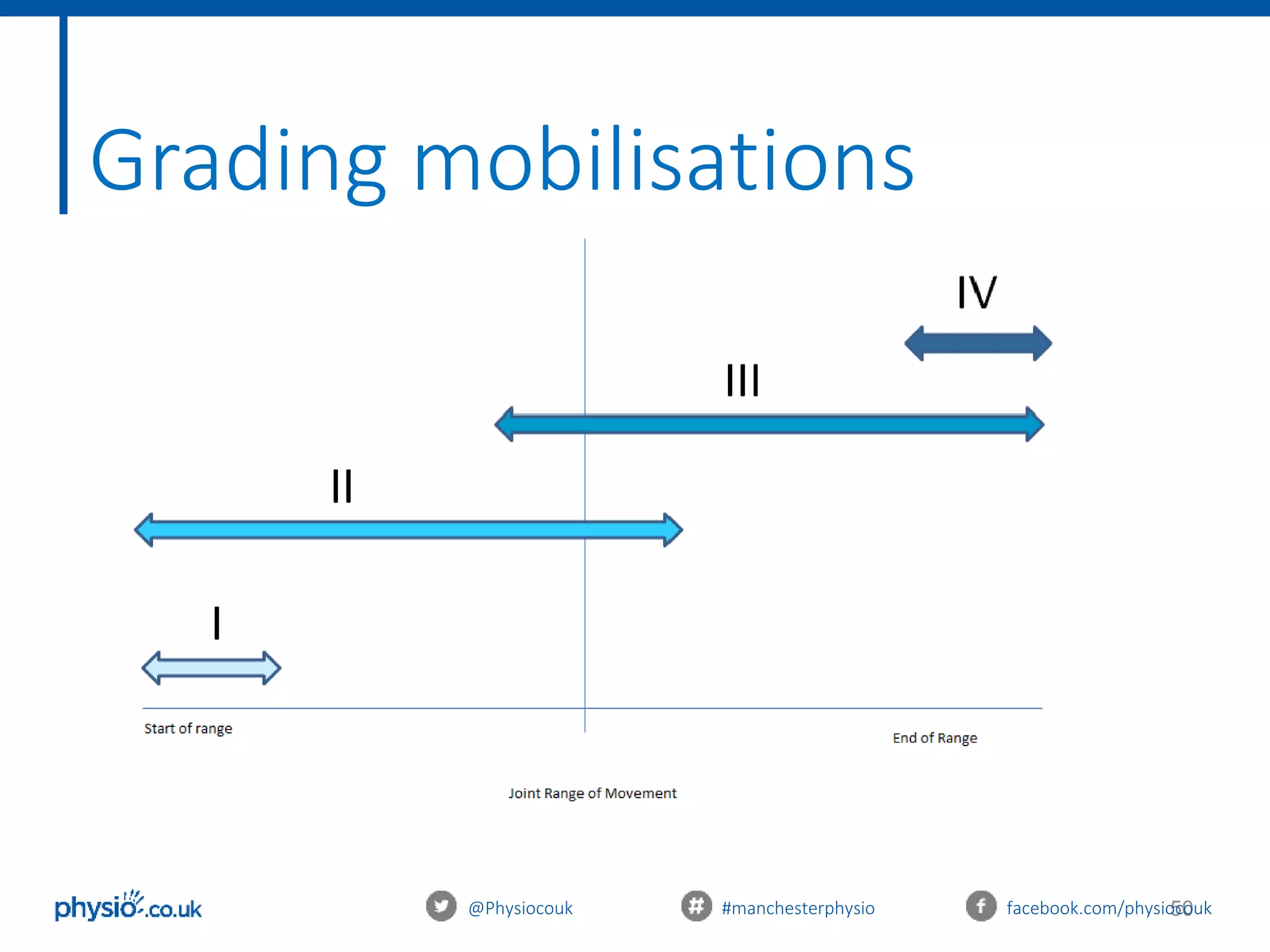
This document provides an introduction to joint mobilization techniques for sports and massage therapists. It begins with an overview of joint anatomy and kinematics, including physiological and accessory movements. Assessment techniques like evaluating range of motion, capsular patterns, and end-feels are described. The aims of mobilizations like restoring range of motion, reducing pain via the pain gate theory, and increasing local blood flow are explained. Precautions and contraindications are listed. Grading of mobilization techniques from grade 1 to 4 are defined based on amplitude and patient pain level. The document concludes with treatment principles to consider for safe and effective joint mobilizations.