Download as PDF, PPTX

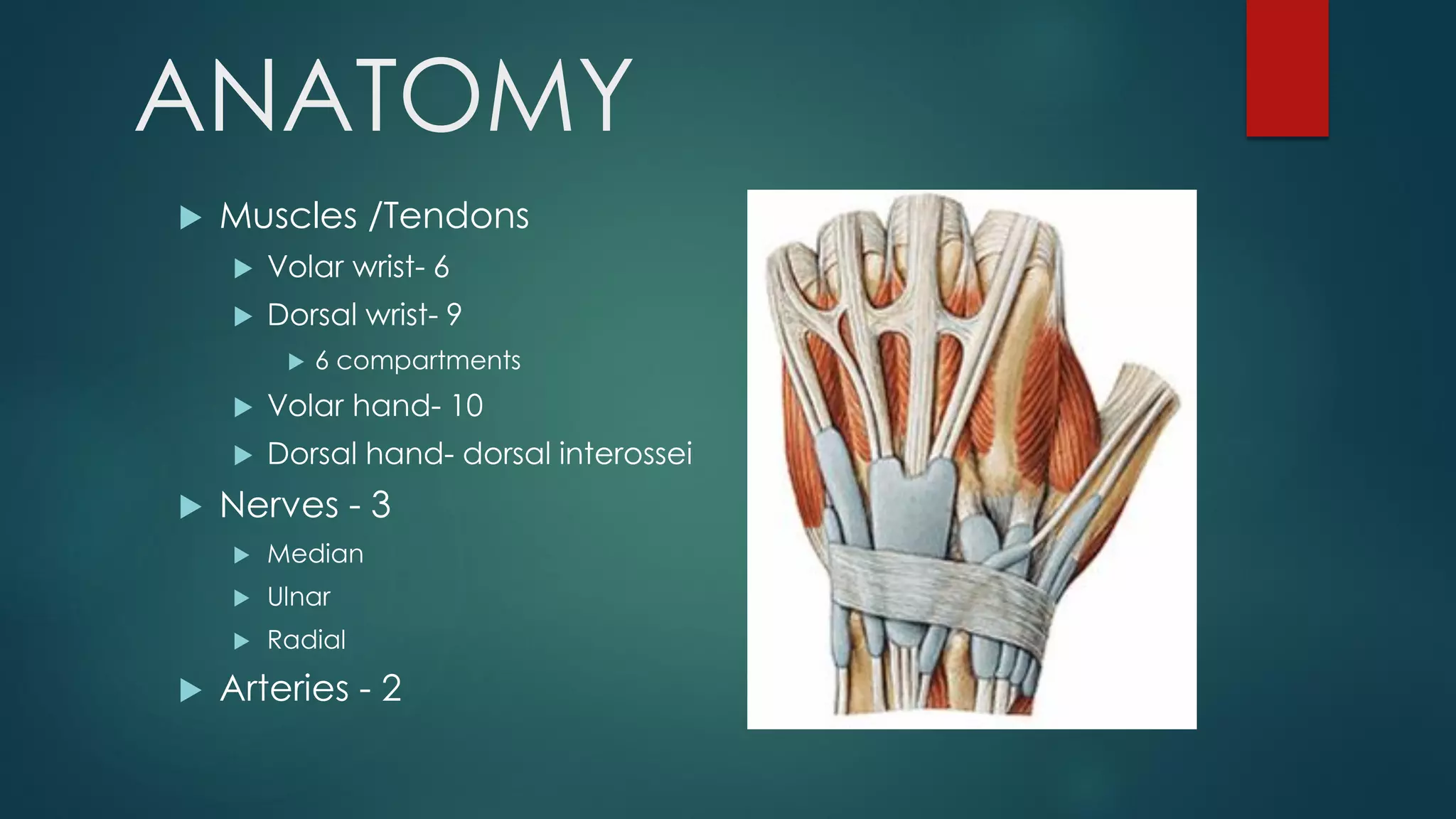
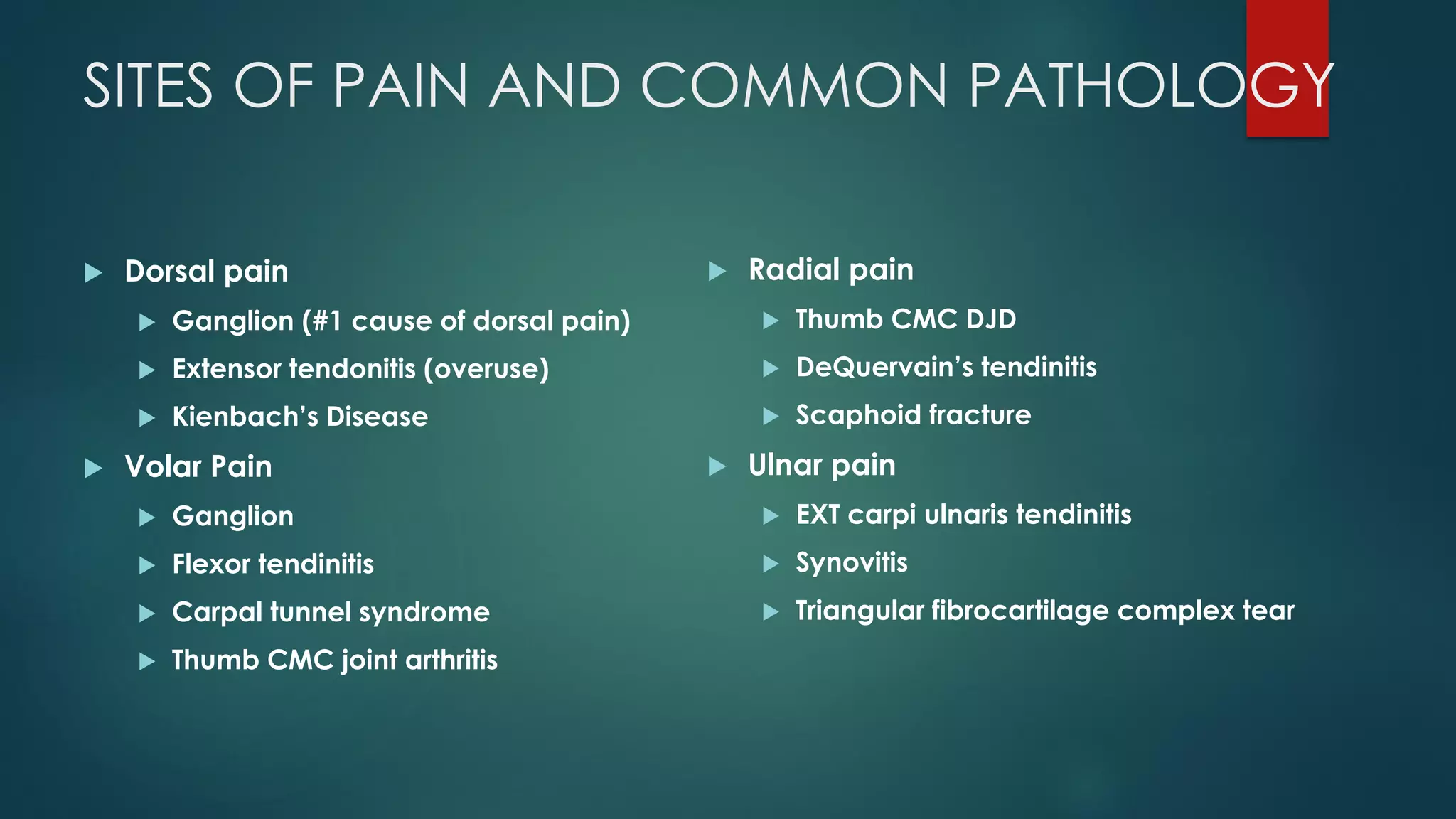
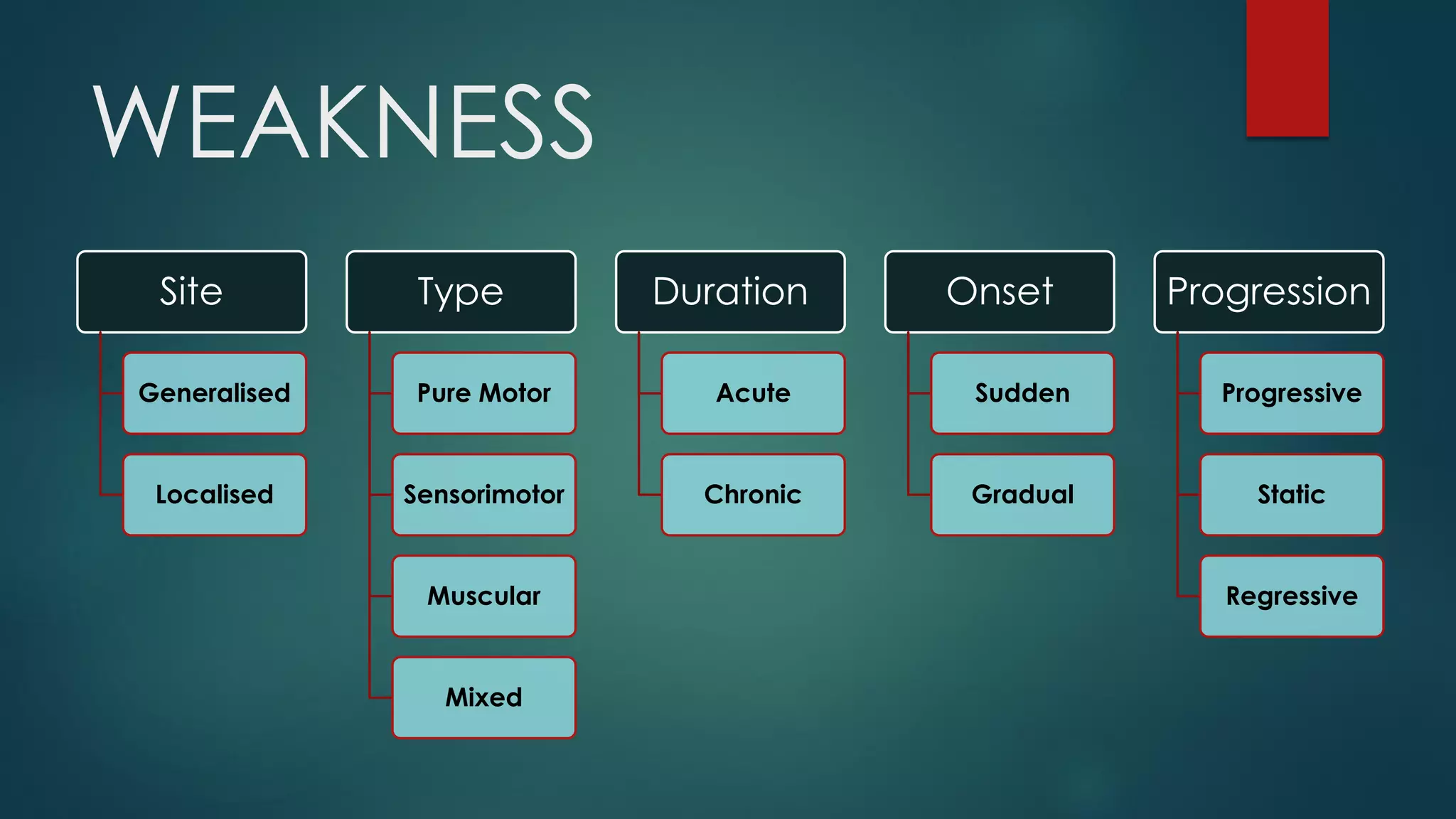
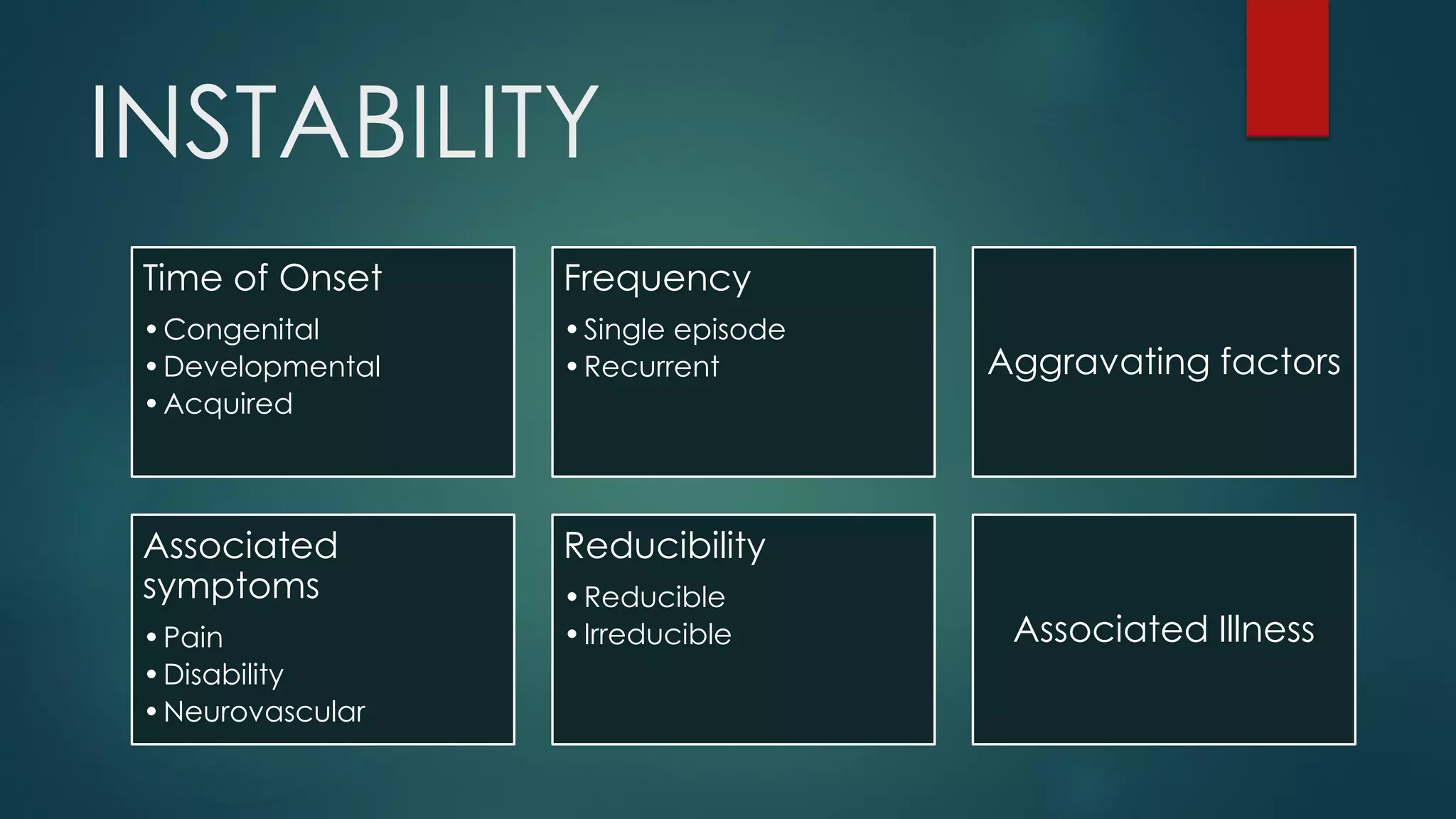
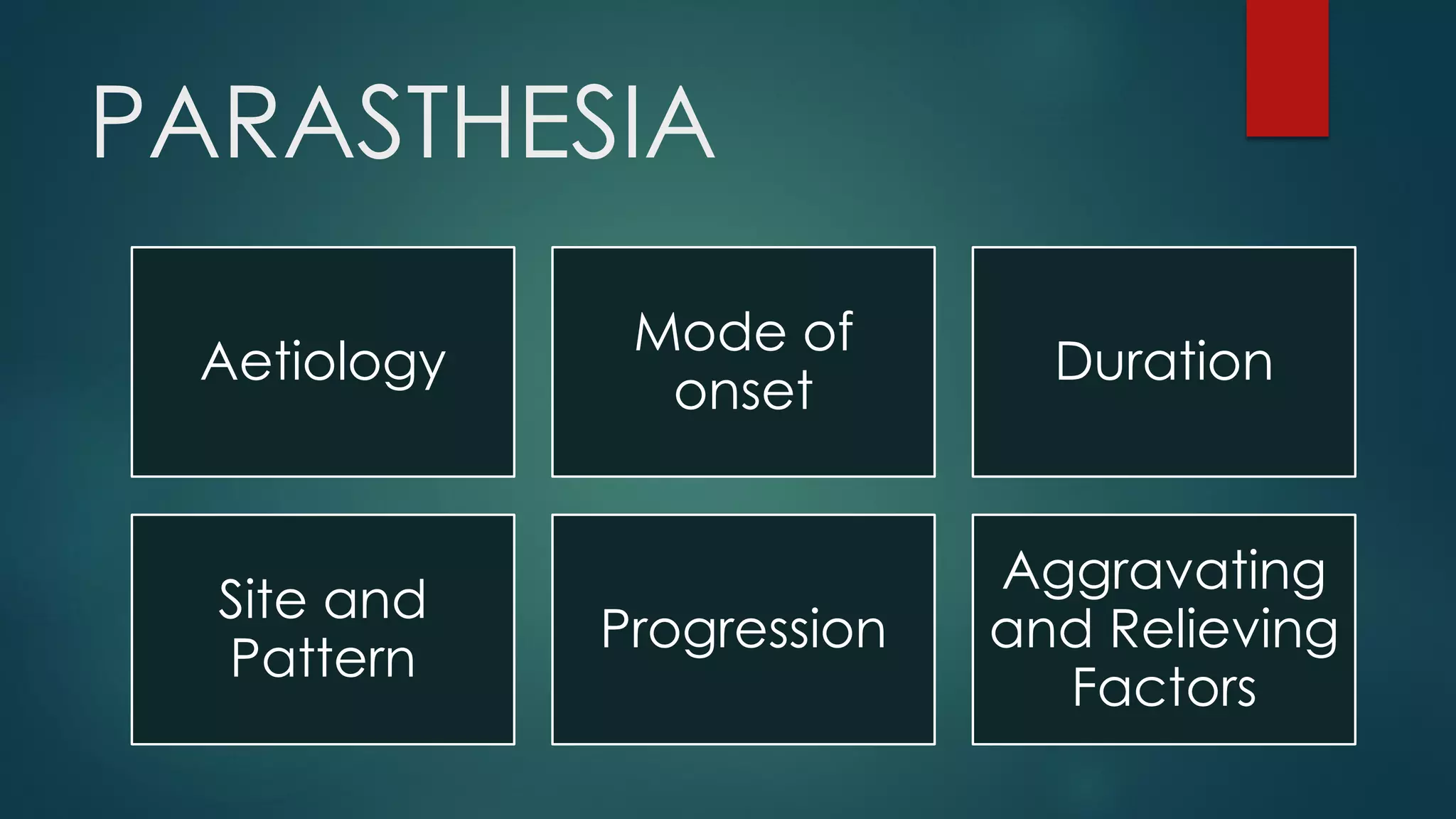
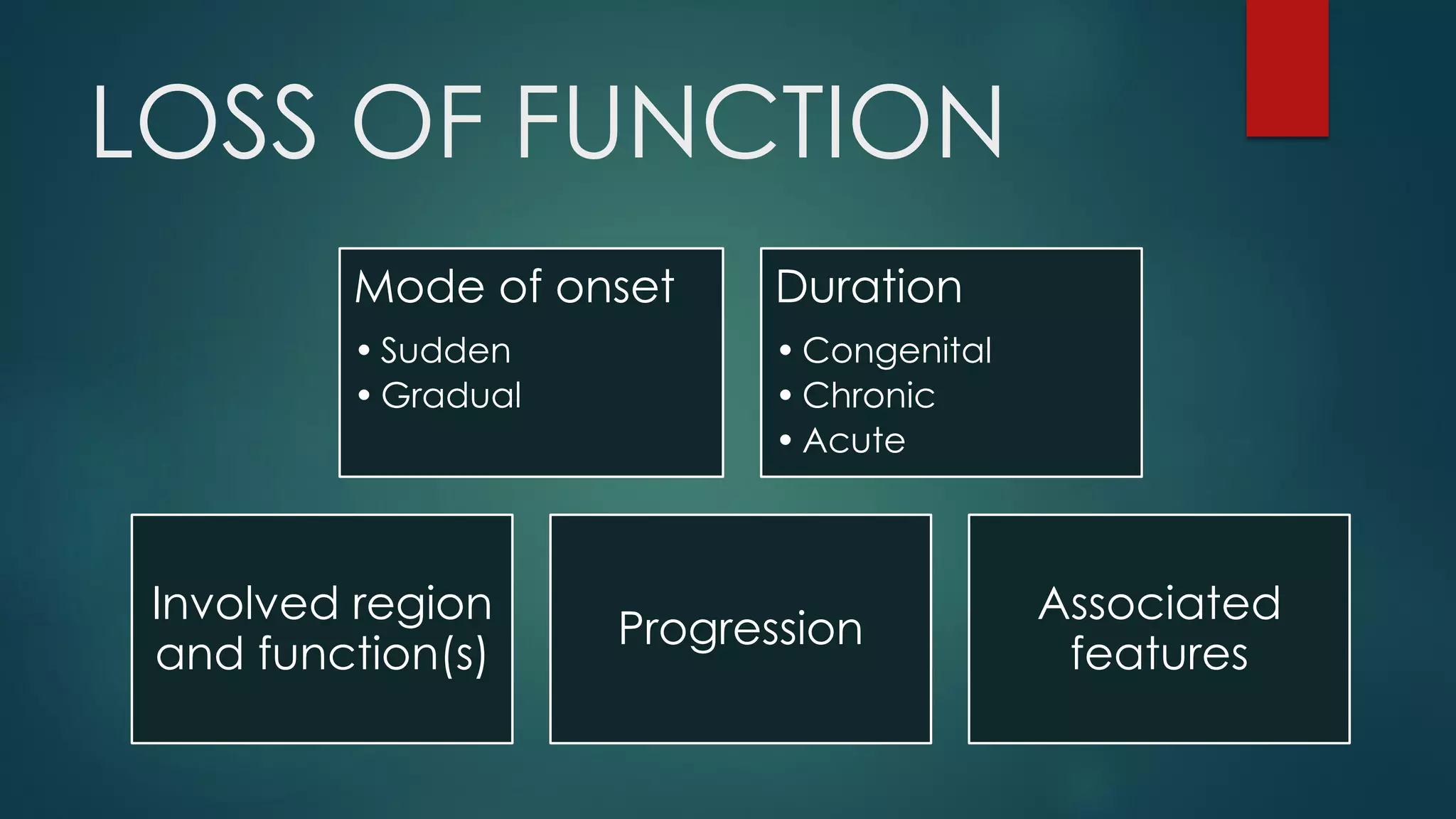


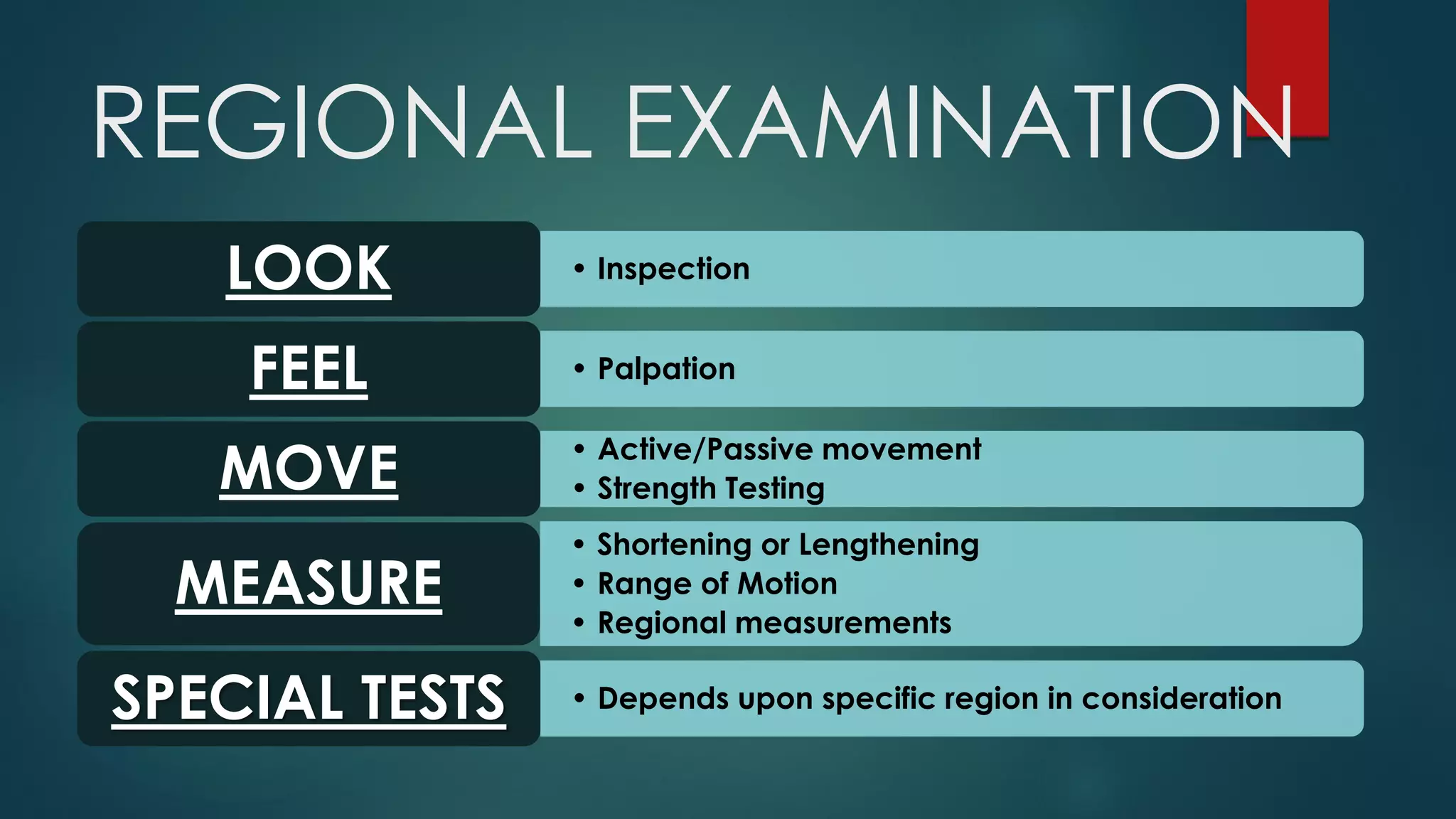
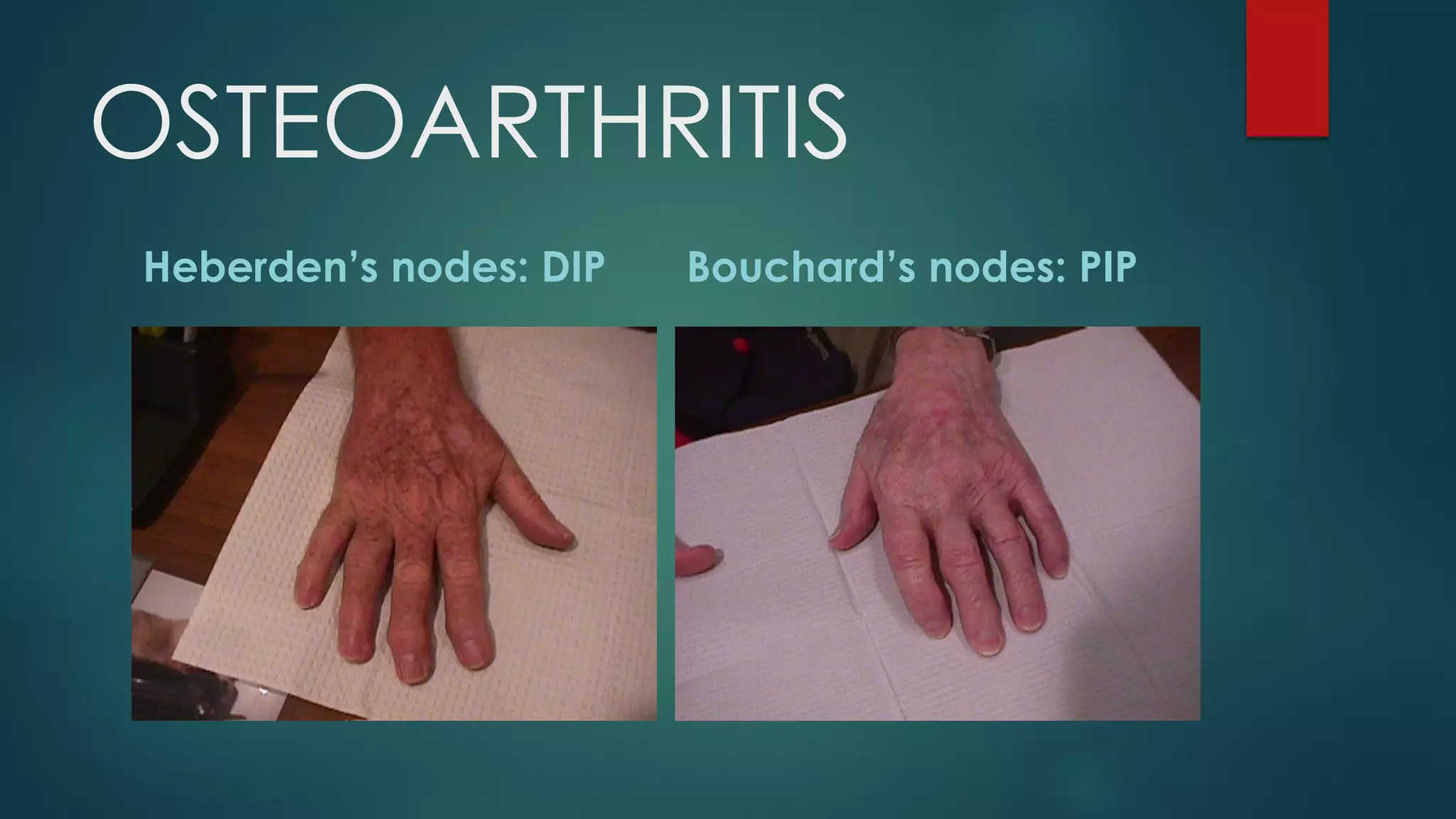
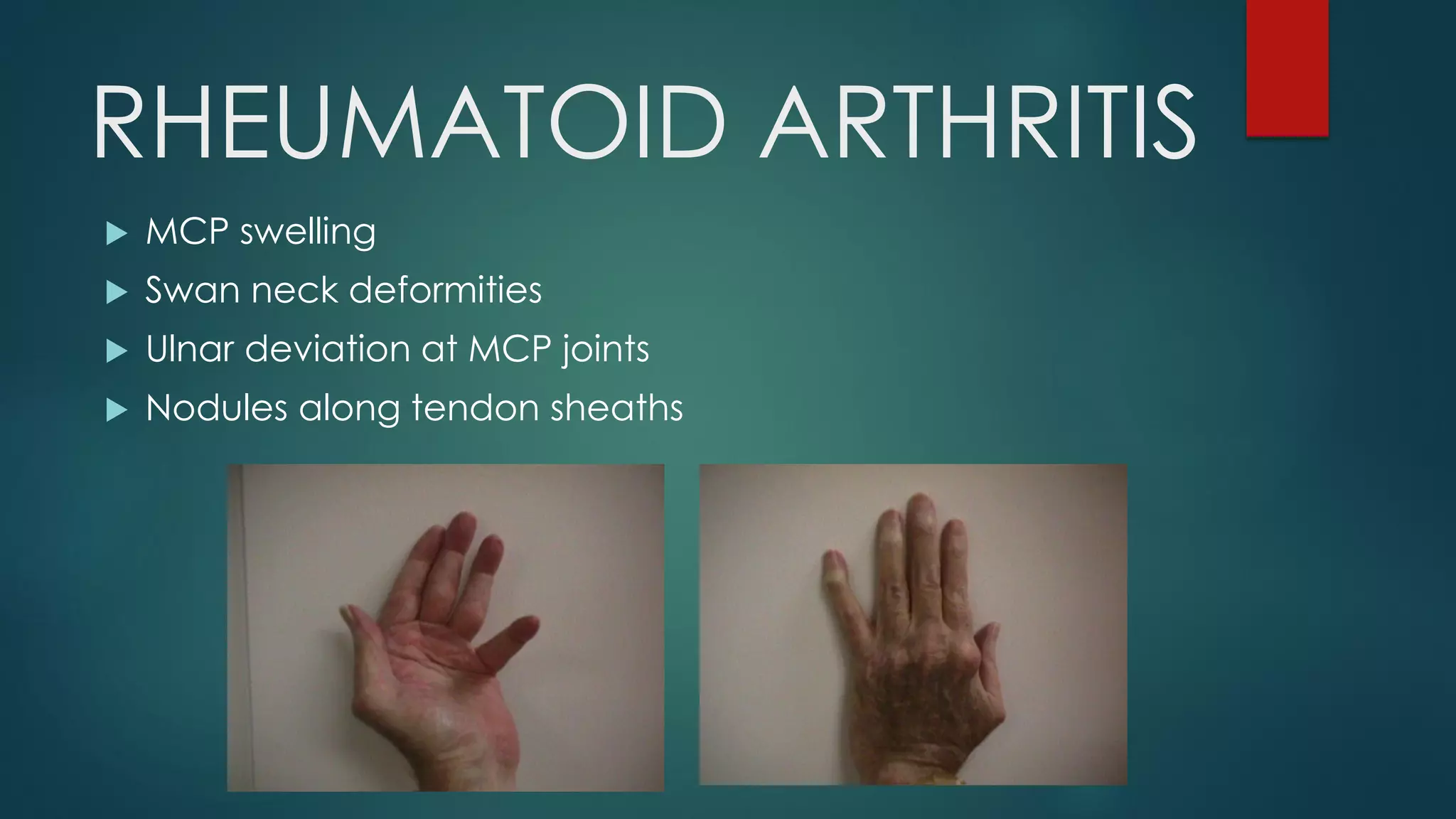
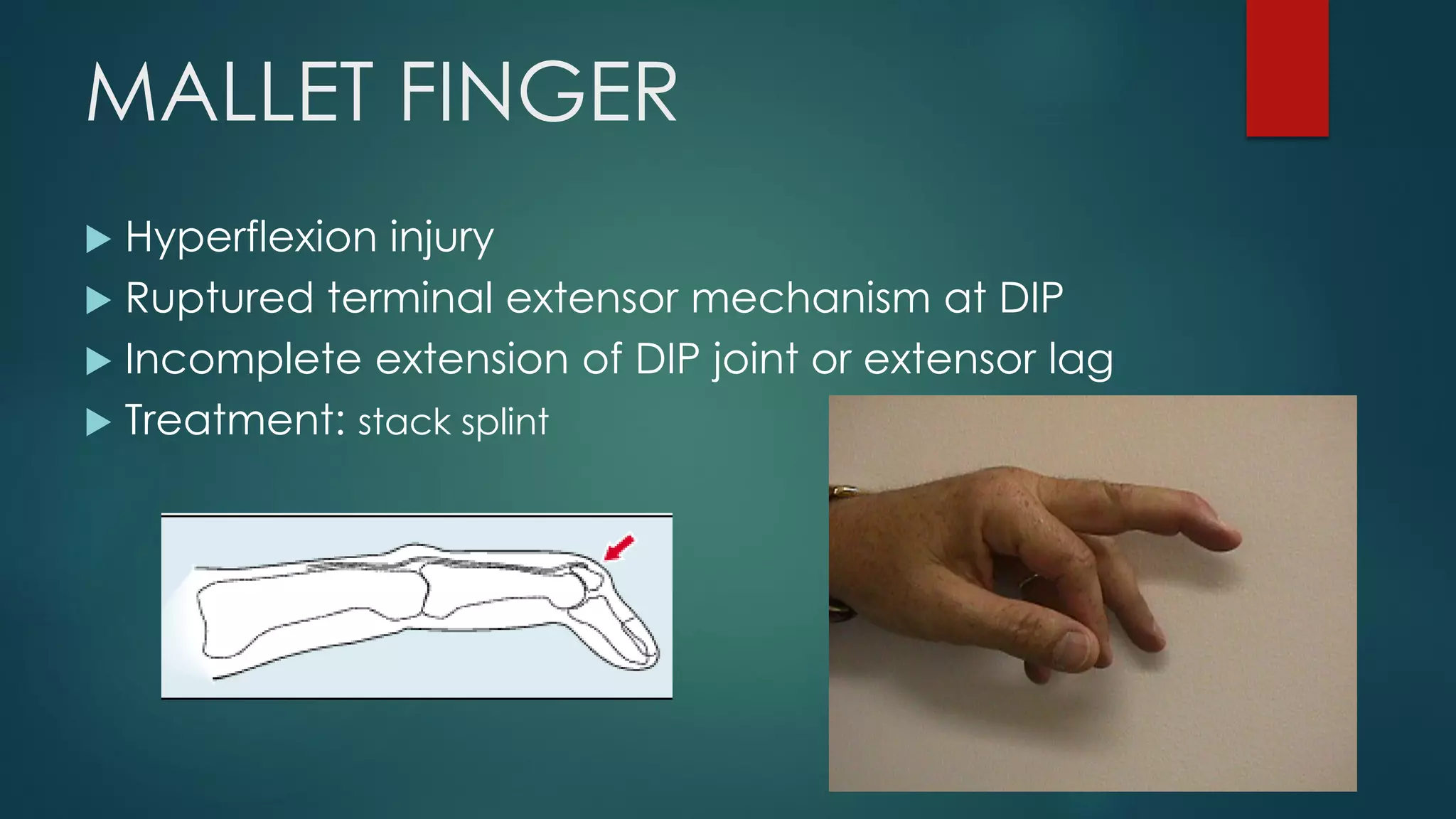
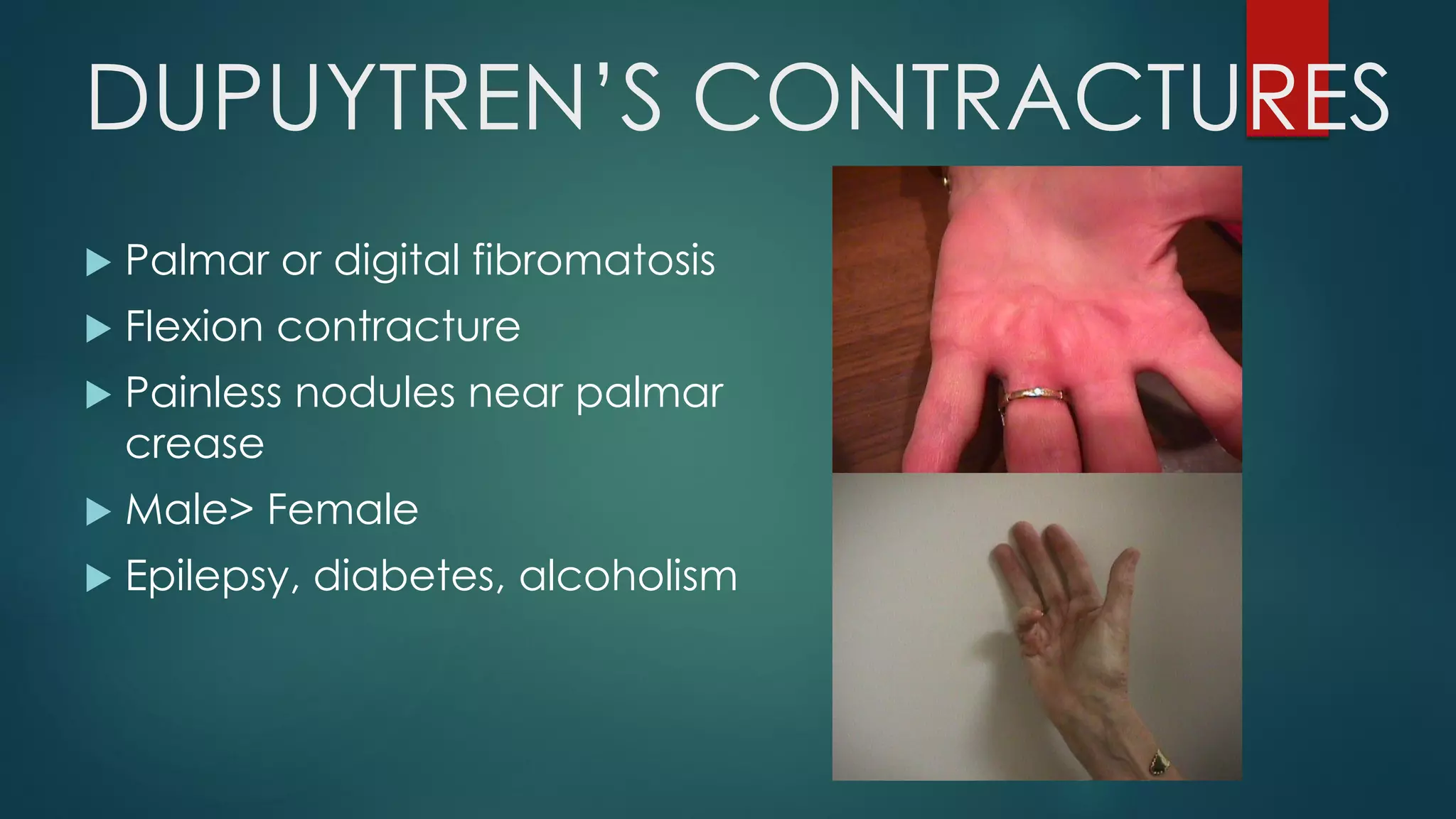
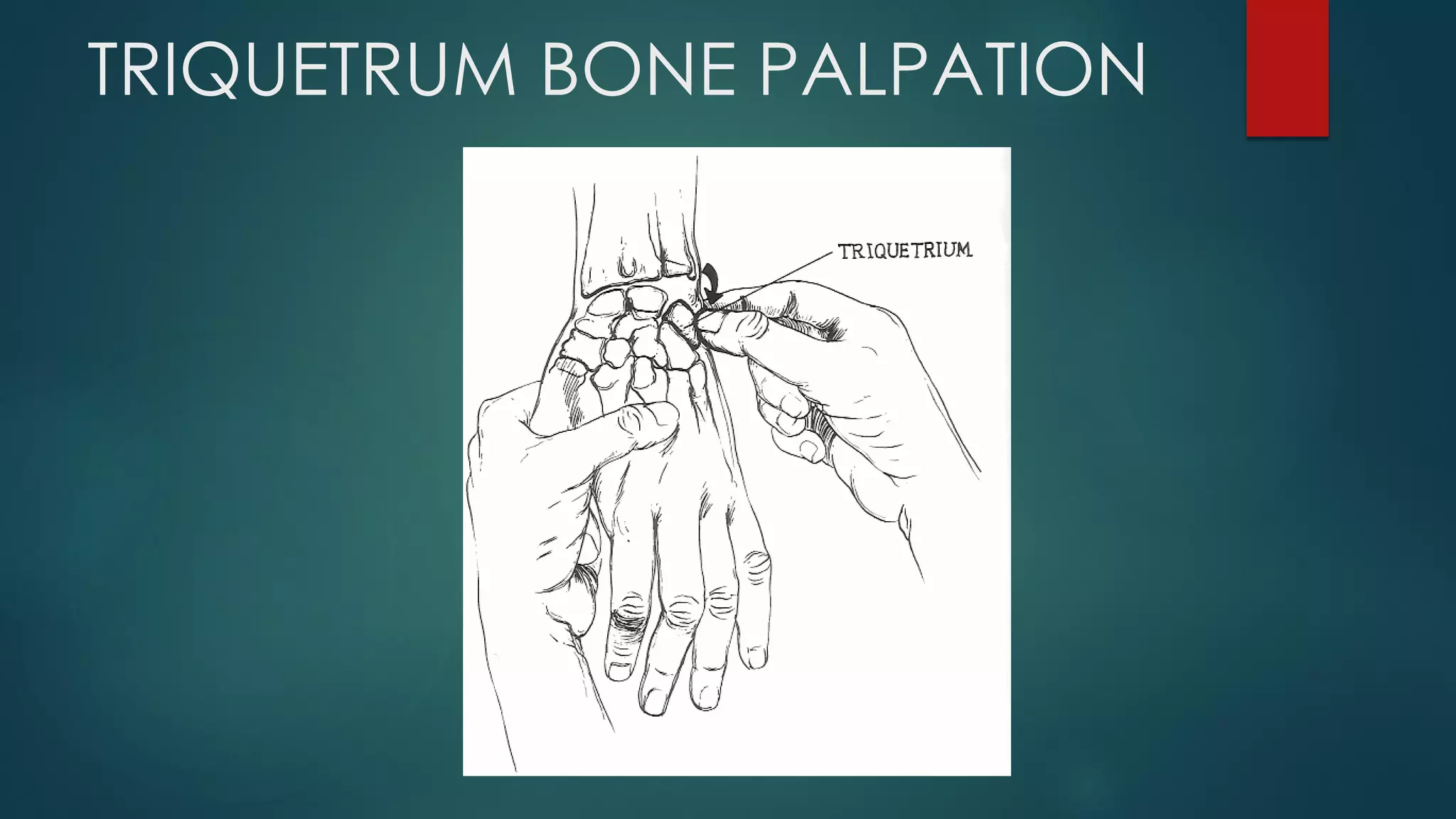
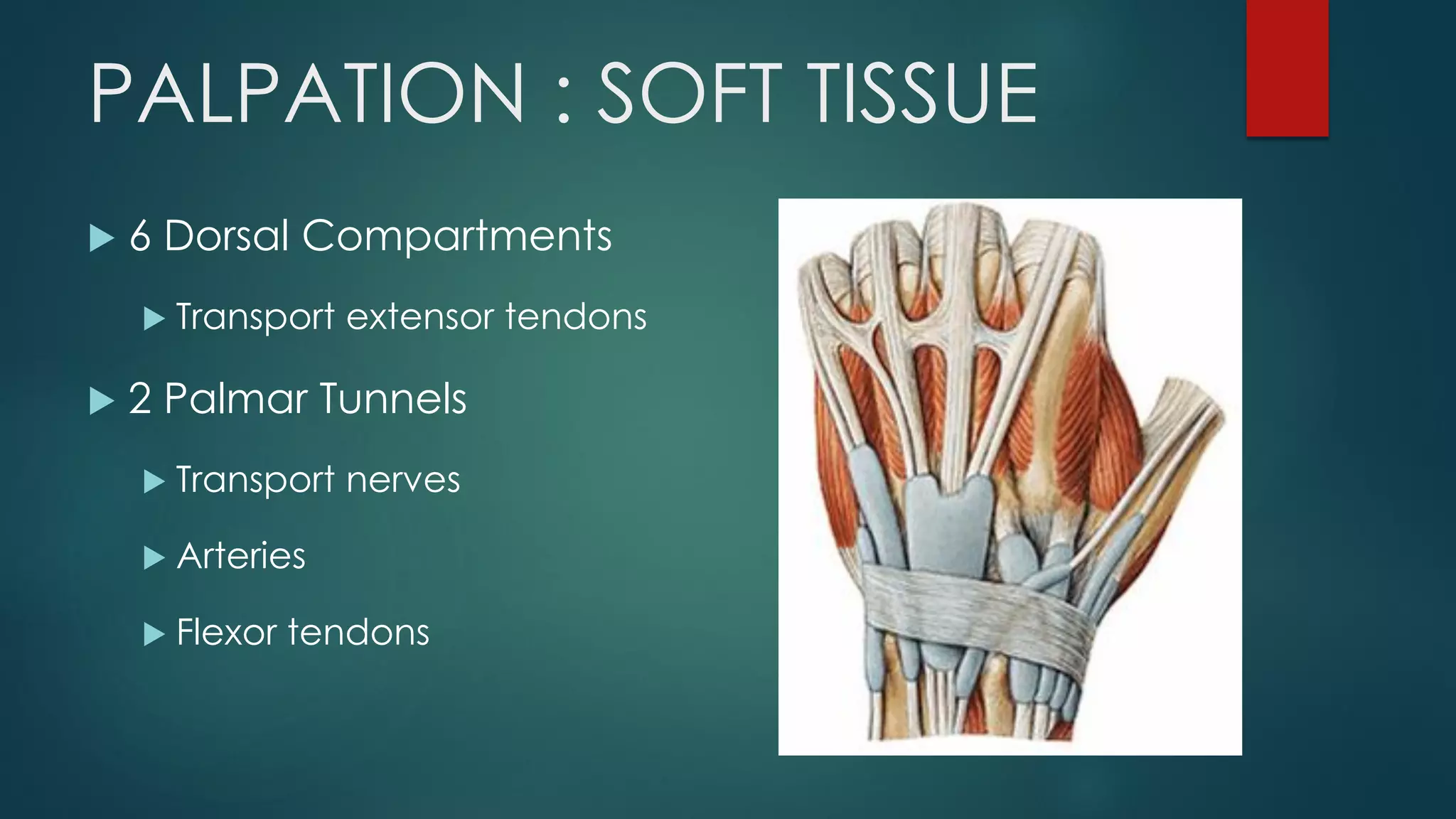

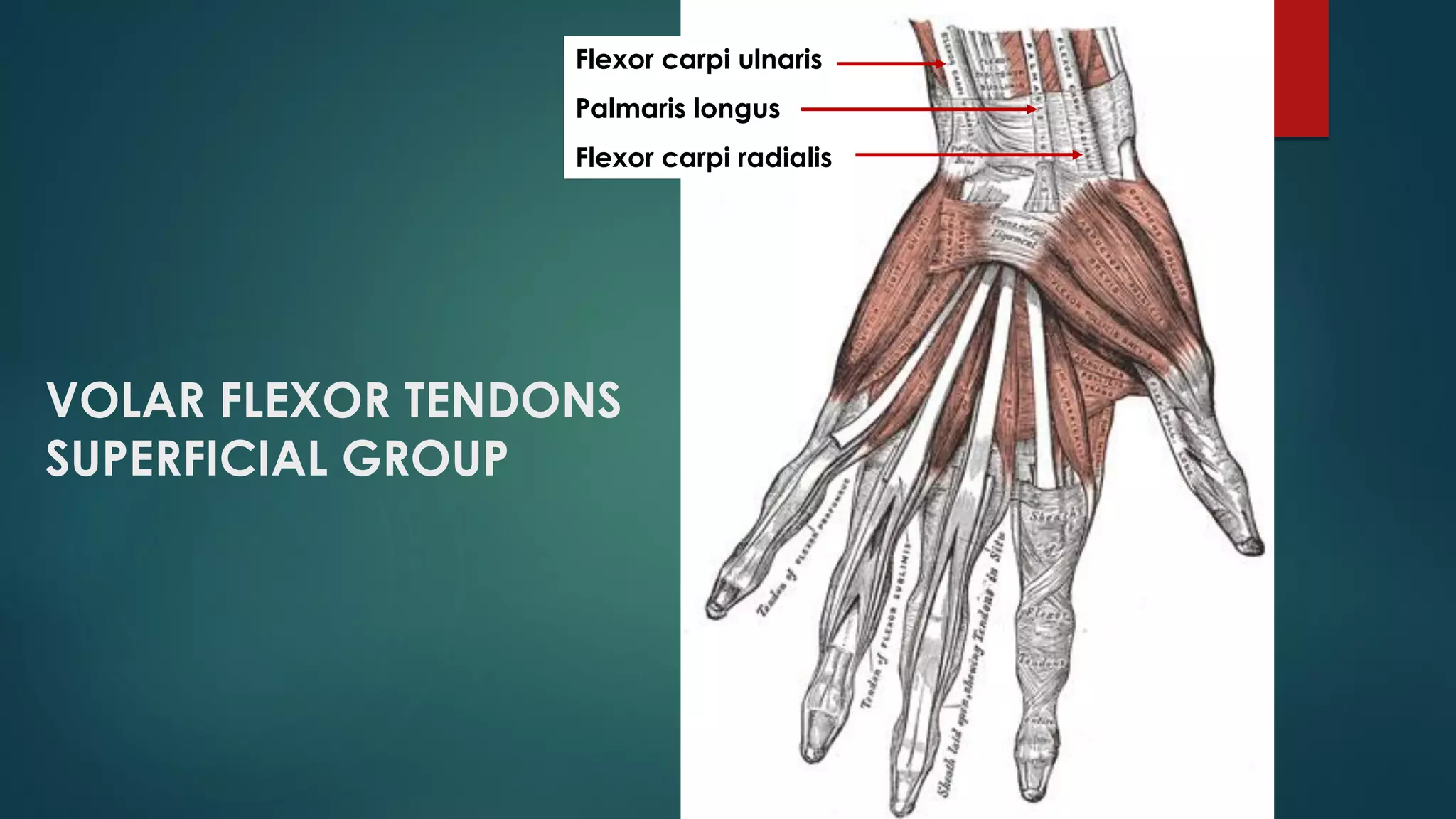

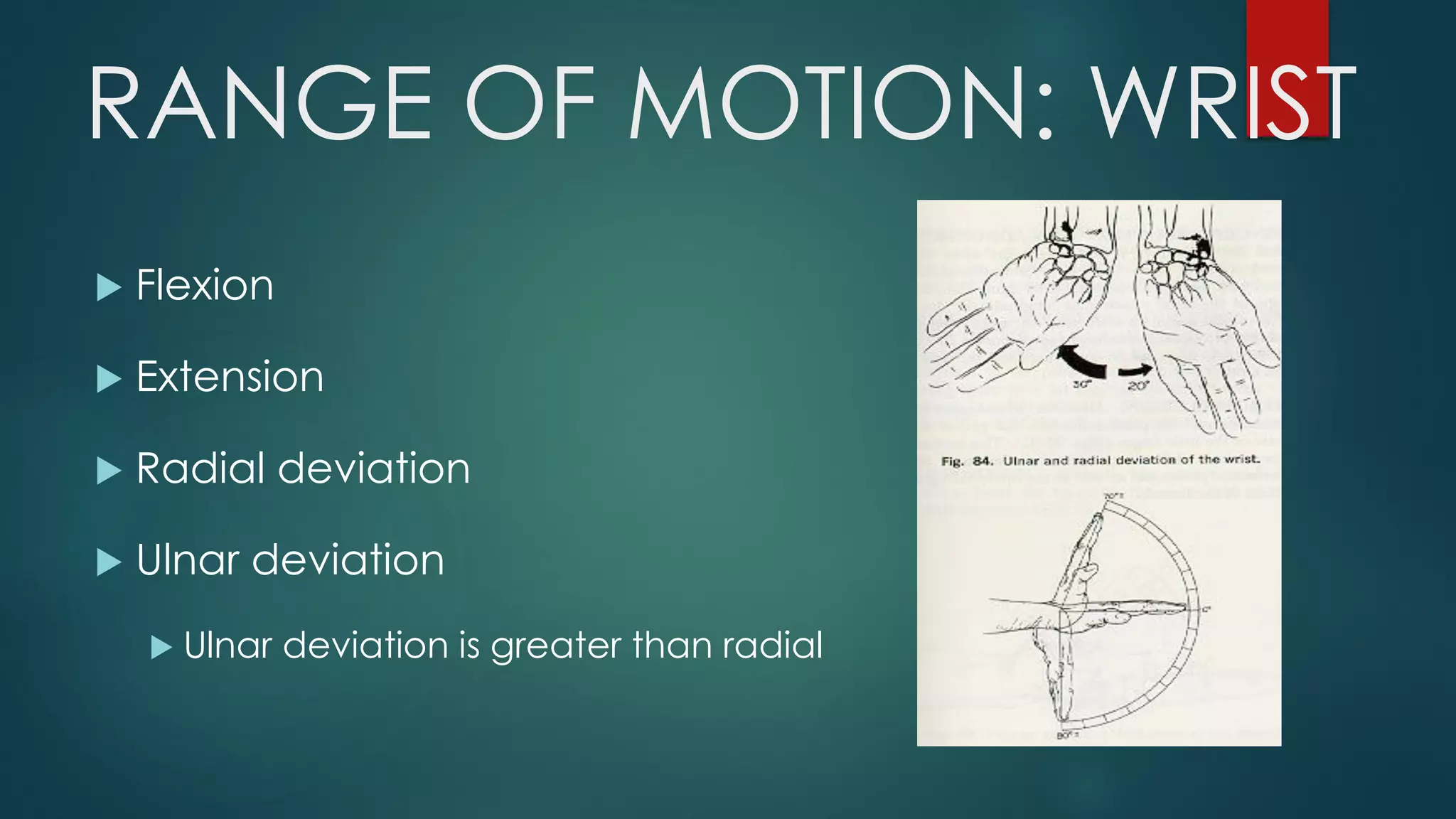


This document provides guidance on evaluating the wrist and hand through history taking and physical examination. It outlines the complex anatomy of the wrist and hand and lists common conditions that may present. The history should explore the chief complaint, past history, mechanisms of injury, and specific symptoms. The physical exam involves inspection, palpation, and assessment of range of motion and strength. Key aspects of the exam are outlined, including tests for certain conditions. Differential diagnoses are provided for various wrist, hand, and finger presentations.























































































