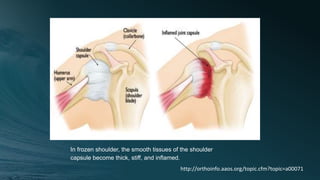
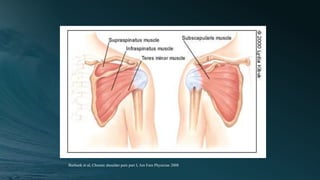
- The document discusses shoulder pain and frozen shoulder. Frozen shoulder progresses through painful freezing and frozen stages as the shoulder capsule becomes inflamed and stiff, limiting range of motion.
- It presents a case of a 48-year-old male with left shoulder pain for 2 months. Exam finds decreased range of motion and pain with abduction. Treatment includes acupuncture at points like ST38 and SI4 to relieve pain and increase range of motion.
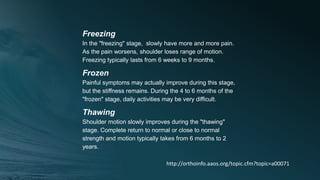
- The stages of frozen shoulder - freezing, frozen, and thawing - are described as the condition progresses from increasing pain and stiffness to gradual improvement in motion over 6 months to 2 years.








![Peripheral Nerves of Upper Limb [Radial, Median & Ulnar nerve]](https://cdn.slidesharecdn.com/ss_thumbnails/sb-190709091558-thumbnail.jpg?width=640&height=640&fit=bounds)





















































































