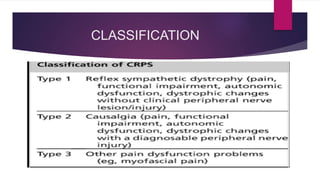
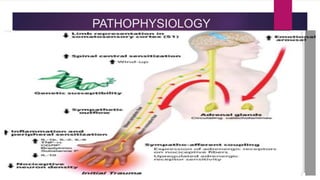
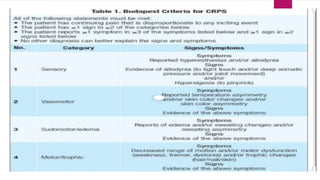
This document provides an overview of Sudeck's osteodystrophy, also known as complex regional pain syndrome. It defines the condition as chronic regional pain disproportionate to any injury, characterized by sensory, motor, and trophic changes. It classifies the condition and outlines risk factors, pathophysiology, staging according to signs and symptoms, diagnostic criteria including bone scans and response to sympathetic blocks, differential diagnosis, and management approaches including pharmacotherapy, nerve stimulation, nerve blocks, sympathectomy. The prognosis is best if treated within the first 3 months to prevent irreversible changes.