Presentation1.pptx, intra cranial vascular malformation.
•Download as PPTX, PDF•
33 likes•3,406 views

This document discusses various pathologies of intra-cranial vascular disease including aneurysms, arteriovenous malformations, cavernous hemangiomas, and Moyamoya disease. It provides details on the prevalence, types, clinical presentation, imaging findings, and treatment of different conditions. In particular, it notes that brain aneurysms are abnormal bulges in brain arteries that can rupture and cause life-threatening bleeding. Imaging tools like CT, MRI, and DSA are used to detect aneurysms and other vascular abnormalities. Moyamoya disease involves progressive stenosis of carotid arteries and formation of collateral vessels visible on angiography.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Presentation1.pptx, intra cranial vascular malformation.
Similar to Presentation1.pptx, intra cranial vascular malformation. (20)
More from Abdellah Nazeer
More from Abdellah Nazeer (20)
Recently uploaded
Recently uploaded (20)
Presentation1.pptx, intra cranial vascular malformation.
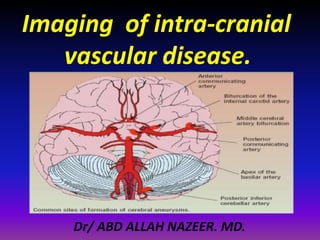
- 1. Imaging of intra-cranial vascular disease. Dr/ ABD ALLAH NAZEER. MD.
- 18. Pathology. Aneurysm. Arterial venous malformation.(AVMs). . Parenchymal(pial) . Dural . Mixed pial-dural Cavernous hemangioma(Cavernoma). Capillary telangiectasias. Venous angioma. Vein of Galen aneurysm. Venous varix. Moyamoya disease.
- 19. A brain aneurysm is an abnormal bulge in a brain artery wall or irreversible dilatation of the arterial that develops where the blood vessel wall is weakened. Lifestyle changes that may be beneficial in preventing a brain aneurysm include: Not smoking Exercising regularly Eating a balanced, low-fat diet Getting help for alcohol and/or drug abuse Controlling high blood pressure Aneurysm
- 20. The prevalence of intracranial saccular aneurysms by radiographic and autopsy series is 5 percent in the United States. Approximately 20 to 30 percent of patients have multiple aneurysms and 70-75% is solitary. Aneurysmal SAH occurs at an estimated rate of 6 to 16 per 100,000 population. Most aneurysms, particularly small aneurysms, do not rupture. Approximately 10 percent of patients die prior to reaching the hospital, and only one-third have a "good result" after treatment. Rupture of an intracranial aneurysm is believed to account for 0.4 to 0.6 percent of all deaths.
- 21. Types: Congenital or acquired. True or false. Acquired (Saccular) with or without systemic disease (ADPKD). Non-saccular- fusiform, dissecting, traumatic, infective , neoplastic and mycotic aneurysm Saccular is the most, occurring at vessel bifurcations. Size varies from a few millimeters to several centimeters.
- 22. By size- . Small aneurysm diameter <1.5 cm. . Large aneurysm(1.5to 2.5 cm). . Giant (2.5to 5 cm). . Super giant (over 5 cm). By Shape- . Saccular, most common: berry aneurysms, necks or stems resembling a berry. . Fusiform- without stem. . Dissecting- blood follows a false lumen.
- 25. Clinical presentation: Most intracranial aneurysms are asymptomatic unless they rupture, and so they are usually found either incidentally or when a patient presents with SAH. The clinical presentation include: 1. rupture(90%) 2. compression from aneurysm sac (7%) 3. Incidental finding (3%)
- 26. Rupture of aneurysm: Headache (97 percent of cases) sudden onset, severe worst headache of my life. Lateralized in 30 percent of patients, predominantly to the side of the aneurysm associated with a brief loss of consciousness, seizure, nausea, vomiting, or meningismus warning leak.
- 27. Incidence: Female: Male = 3:2 But the ratio varies with age: < 40 years: males > females > 40 years: females > males The sites different from gender: female supraclinoid segment of the internal carotid artery. male anterior communicating complex Age: rupture is most common between 40 and 60 years but can occur in any age, even in old age.
- 28. Hereditary syndromes Heritable disorders associated with the presence of intracranial aneurysm include: Connective tissue diseases such as Ehlers-Danlos syndrome and pseudoxanthoma elasticum Autosomal dominant polycystic kidney disease Glucocorticoid-remediable aldosteronism (familial aldosteronism type I). Familial aneurysms Familial aneurysms tend to rupture at a smaller size and younger age than sporadic aneurysms. Siblings often experience rupture in the same decade of life.
- 29. CT: An unenhanced CT scan is the preferred procedure for detection of SAH is positive in more than 90% of patients in the first 24 hours more than 50% in the first week the sensitivity drops off dramatically after the first week SAH appears as areas of increased density in the subarachnoid spaces along the base of the skull and within the sylvian fissure. The location of the SAH may frequently suggest the site of the aneurysm, and, rarely, the aneurysm itself might be visible.
- 30. Right MCA aneurysm with subarachnoid hemorrhage.
- 31. 2 cases with subarachnoid hemorrhage from rupture of an aneurysm.
- 32. Computed tomographic (CT) angiography of the head showed a partially thrombosed giant paraclinoid aneurysm of the left internal carotid artery, measuring 5 cm in diameter.
- 33. CTA with MIP and aneurysms of the anterior communicating artery.
- 34. MRI: MRI is not recommended in the acute management of patients with SAH, difficult to manage acutely sick patients within the environment of an MRI suite SAH is poorly seen on MRI, However, for patients with un-ruptured aneurysms MRI and MRA are excellent screening procedures to detect and follow intracranial aneurysms as small as 3 mm have been identified in high-quality MRI studies.
- 37. MCA aneurysm.
- 38. Giant partially thrombosed ICA aneurysm with some calcification at the ventral rim.
- 39. Giant vertebral aneurysm in the vertebral artery with nausea and vomiting due to brain stem compression.
- 40. DSA with small aneurysm at PCA.
- 41. </body Cavernous angioma with left middle cerebral artery aneurysm.
- 63. Cavernoma with signs of recent hemorrhage.
- 74. Vein of Galen malformation.
- 77. Moyamoya syndrome is characterized by progressive stenosis of the internal carotid arteries and formation of collateral vessels that give a "puff of smoke" appearance on angiography. Moyamoya disease occurs mainly in Japanese and other Asian populations and may have a genetic basis and first described at 1957. Secondary moyamoya syndrome is seen in association with neurofibromatosis, Down syndrome, Williams syndrome, sickle cell disease, and as a sequale of cranial irradiation. Intracranial hemorrhage is common in young adults. Dissection — Arterial dissection is the most common vascular abnormality in some young adult series Moyamoya
- 78. Clinical features. Ischemic events more frequent in children. Hemorrhagic stroke Epilepsy. In children: 77%-ischemic events 59%-TIA 5%-ICH In adults: 69%-ICH 27%-TIA +ischemic stroke Epilepsy: 25%- children , 5% -adults.