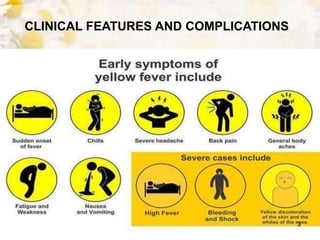
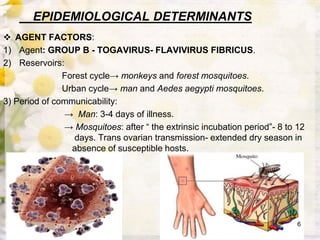
This document discusses yellow fever, a viral hemorrhagic disease transmitted by Aedes mosquitoes. It is caused by a flavivirus that primarily affects monkeys but can infect humans. The disease causes liver and kidney damage that can lead to jaundice, hemorrhaging, and death in 20-50% of cases. It is found in tropical areas of Africa and South America. Prevention relies on vaccination and controlling the Aedes aegypti mosquito vector through environmental management and insecticides.


























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









