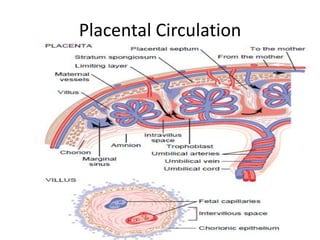
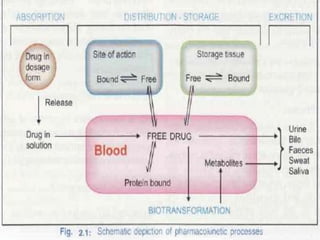
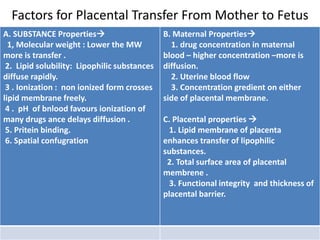
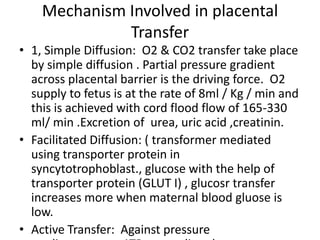
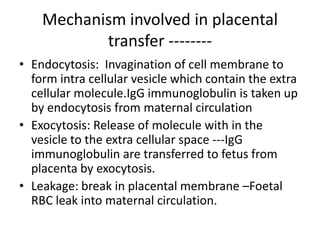
The placental blood barrier protects the fetus from potentially harmful substances in the mother's bloodstream. Most substances over 500 Daltons cannot cross the barrier, though some like antibodies can pass through via endocytosis or pinocytosis. During pregnancy, the placental barrier can allow maternal infections or drugs to impact the fetus. The factors that influence placental transfer from mother to fetus include substance properties like molecular weight and lipid solubility, as well as maternal and placental properties. Nutrients are transferred via simple diffusion, facilitated diffusion using transporter proteins, or active transport against gradients. The placenta also functions as an endocrine gland and provides immunological protection for the fetus.