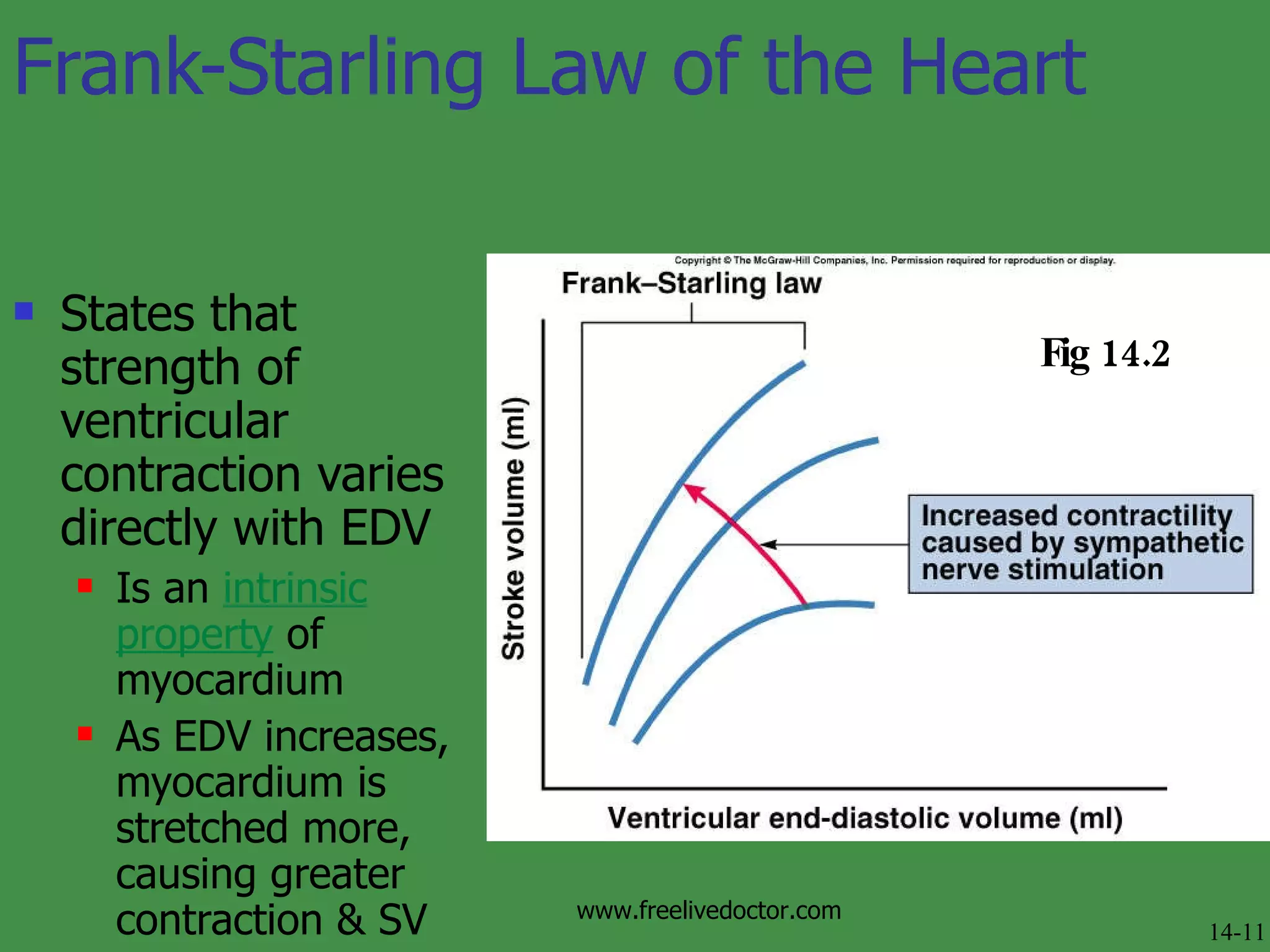
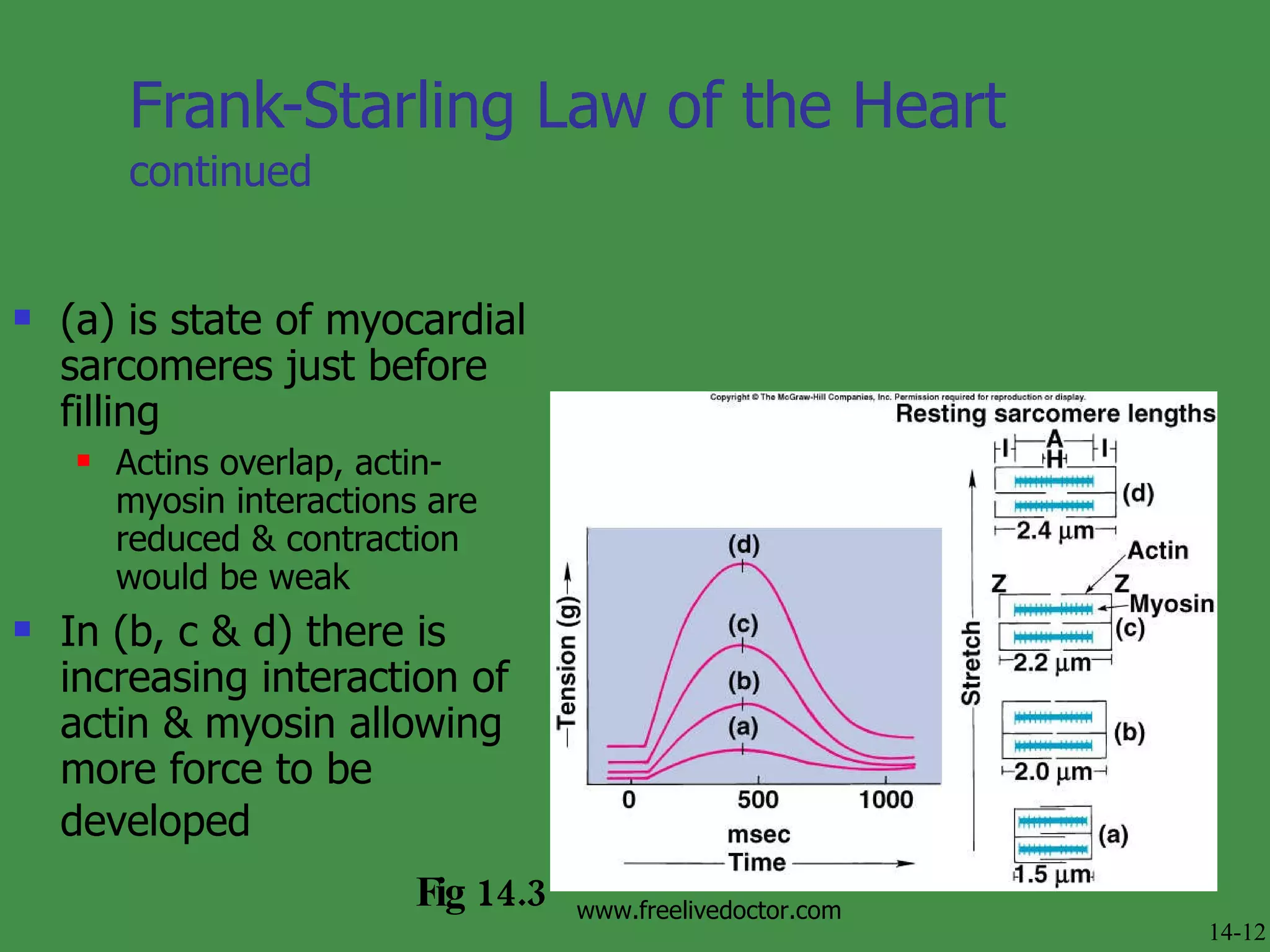
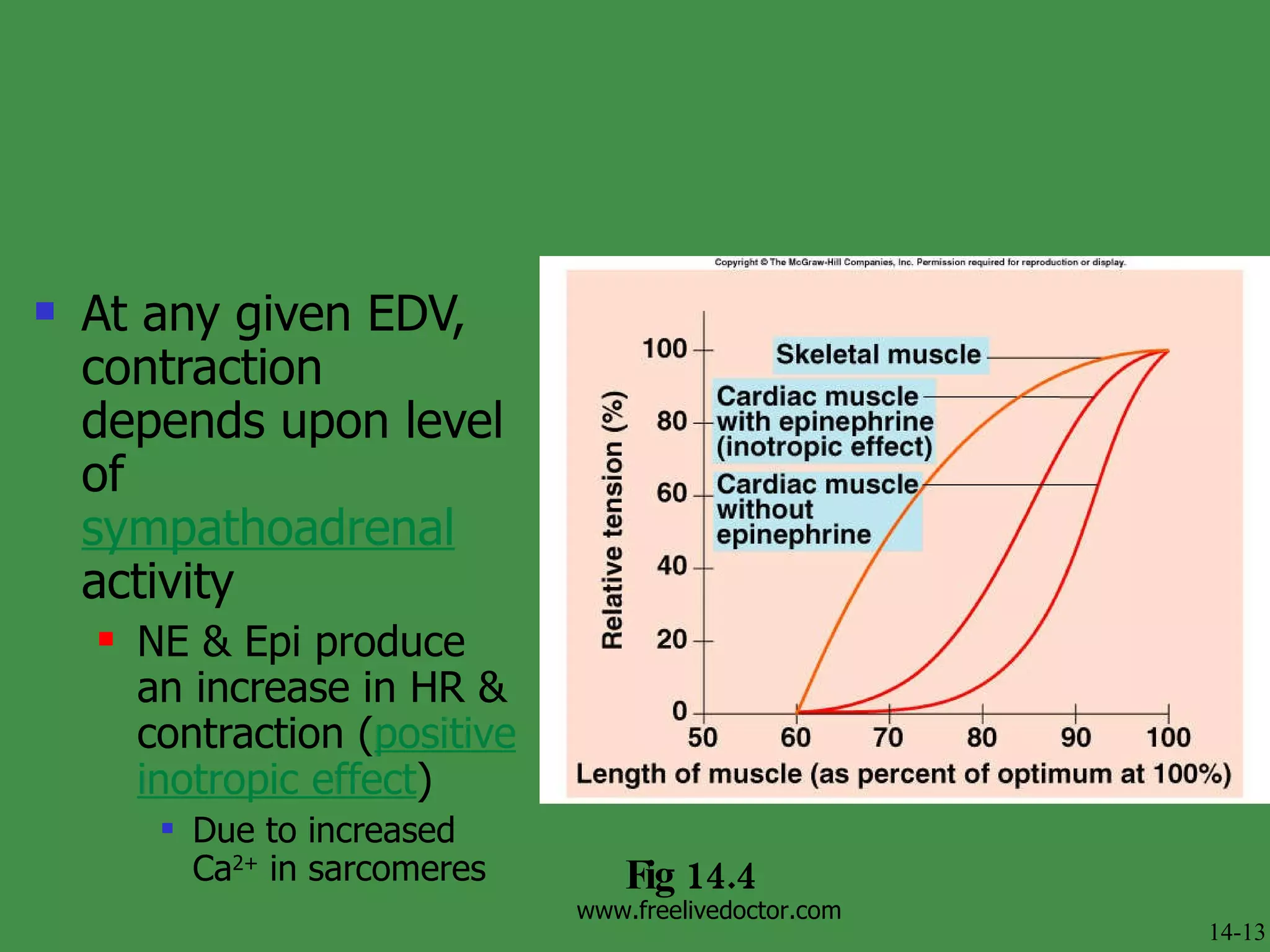
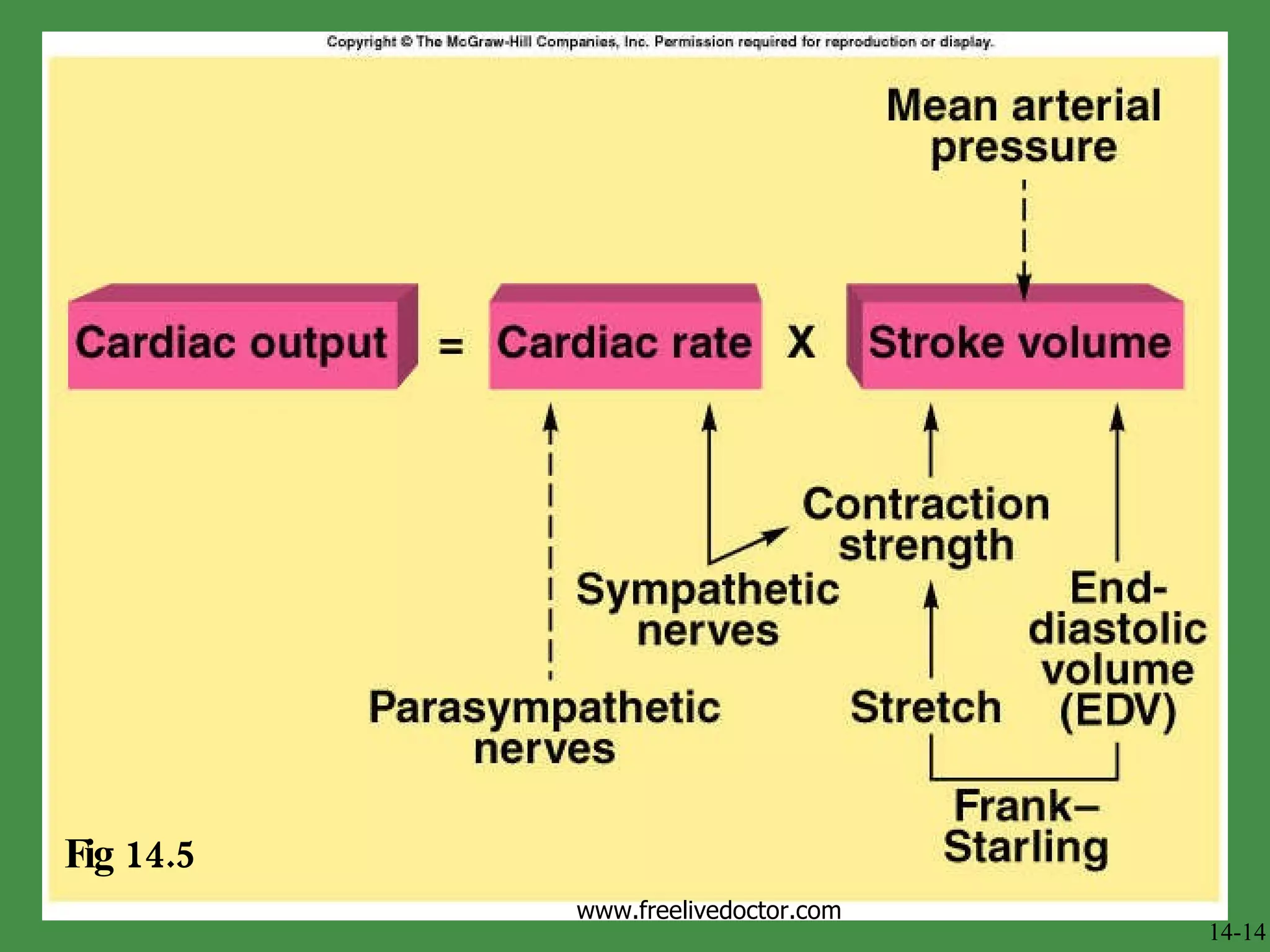
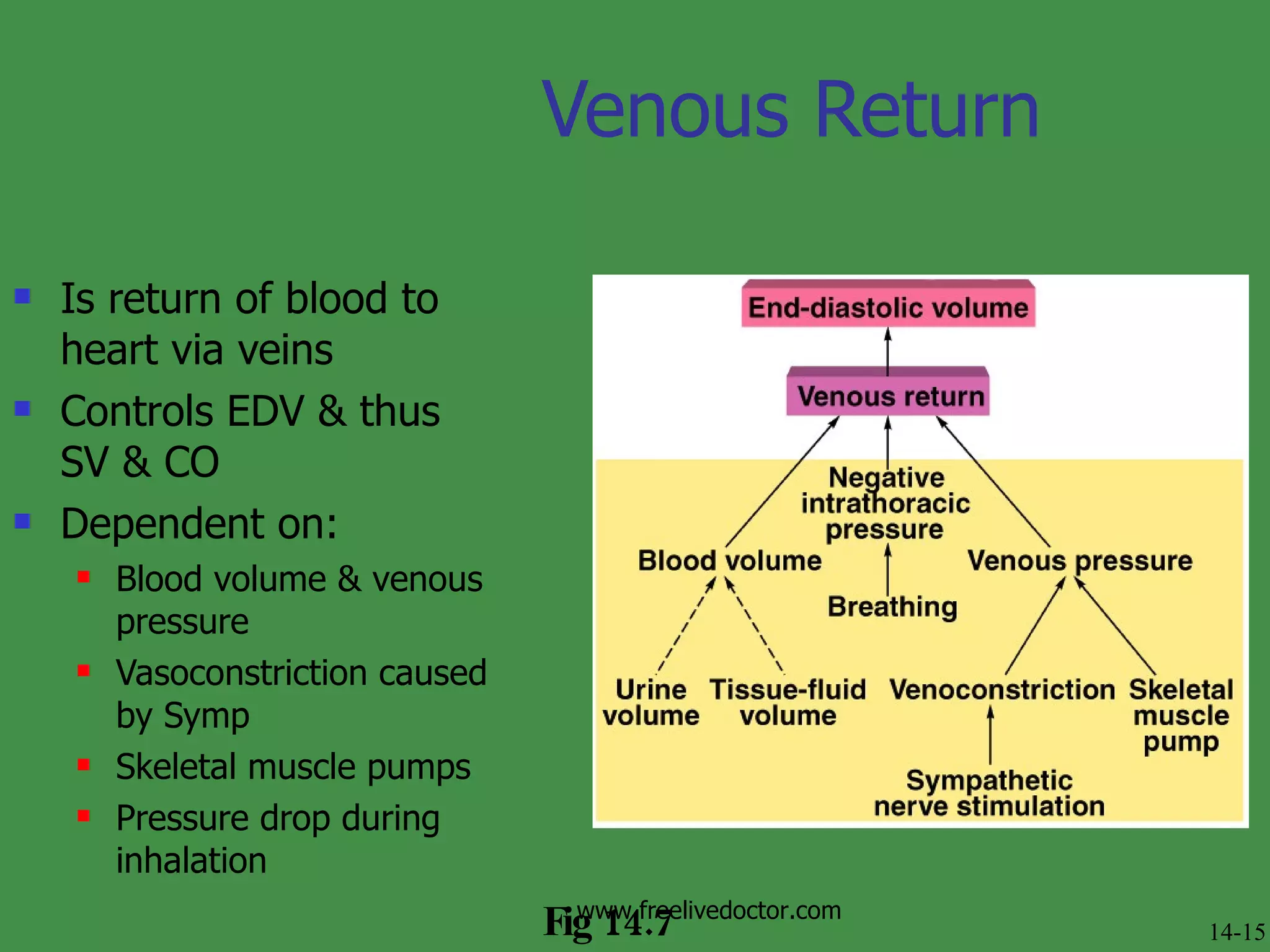
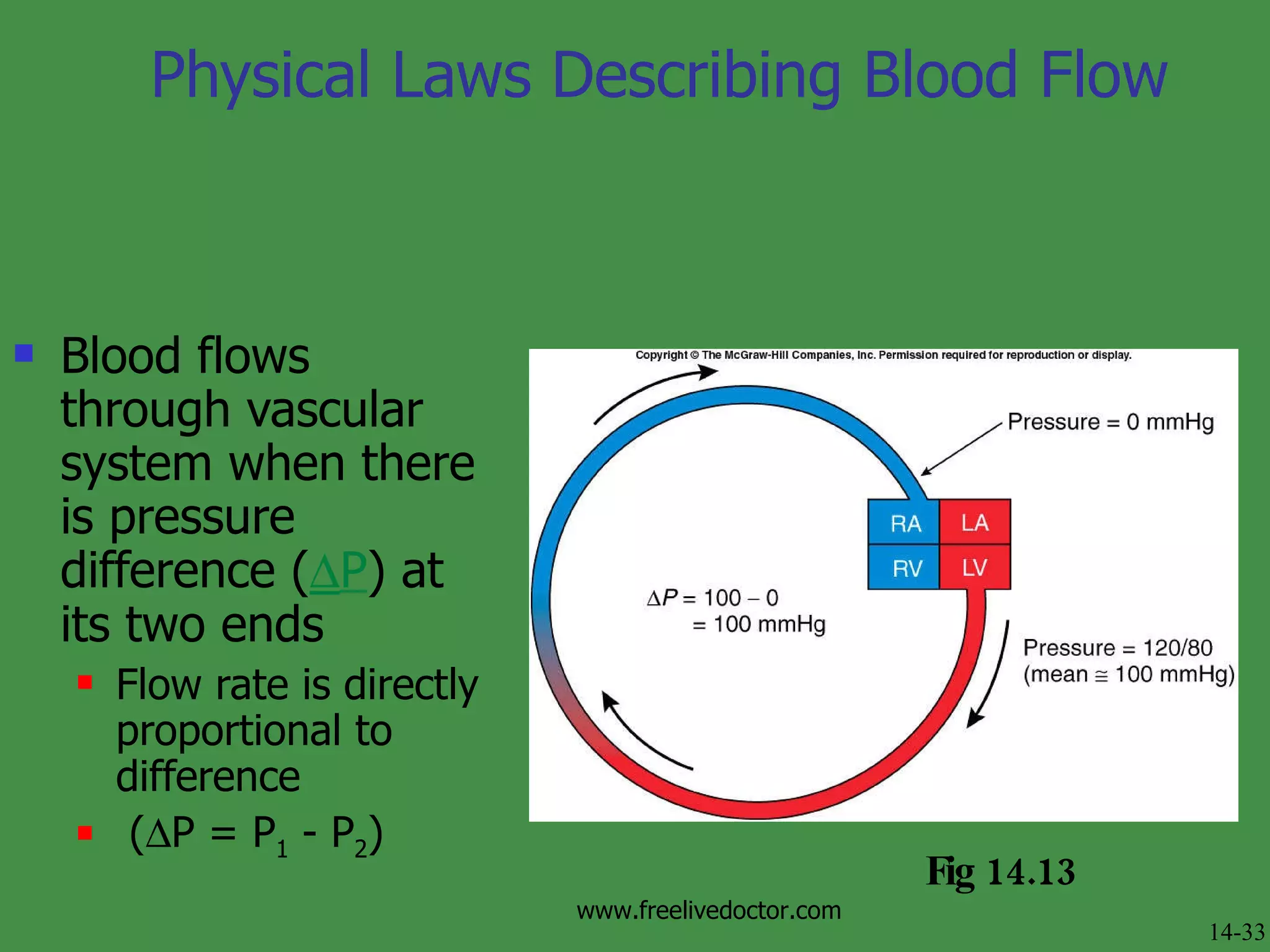
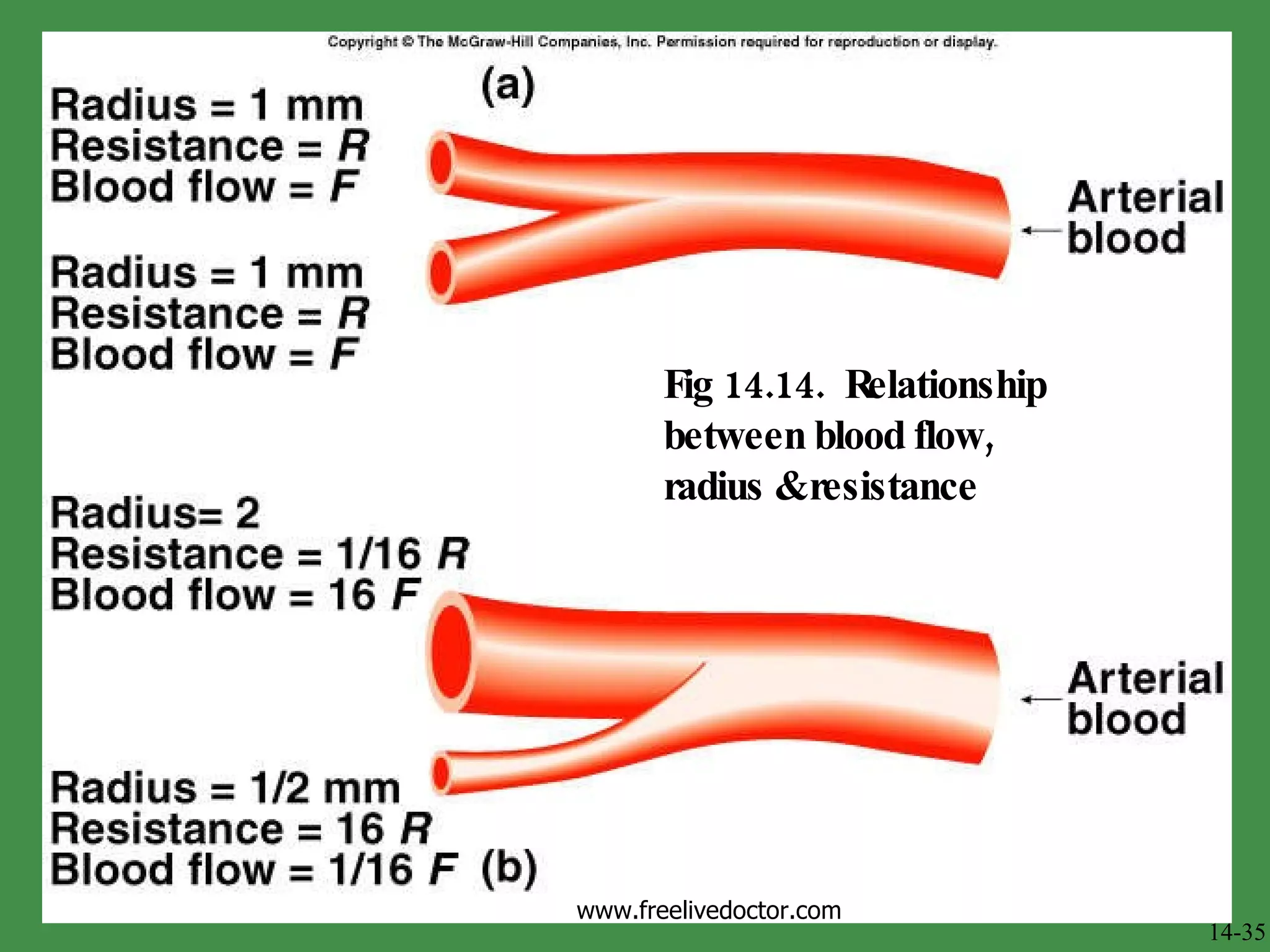
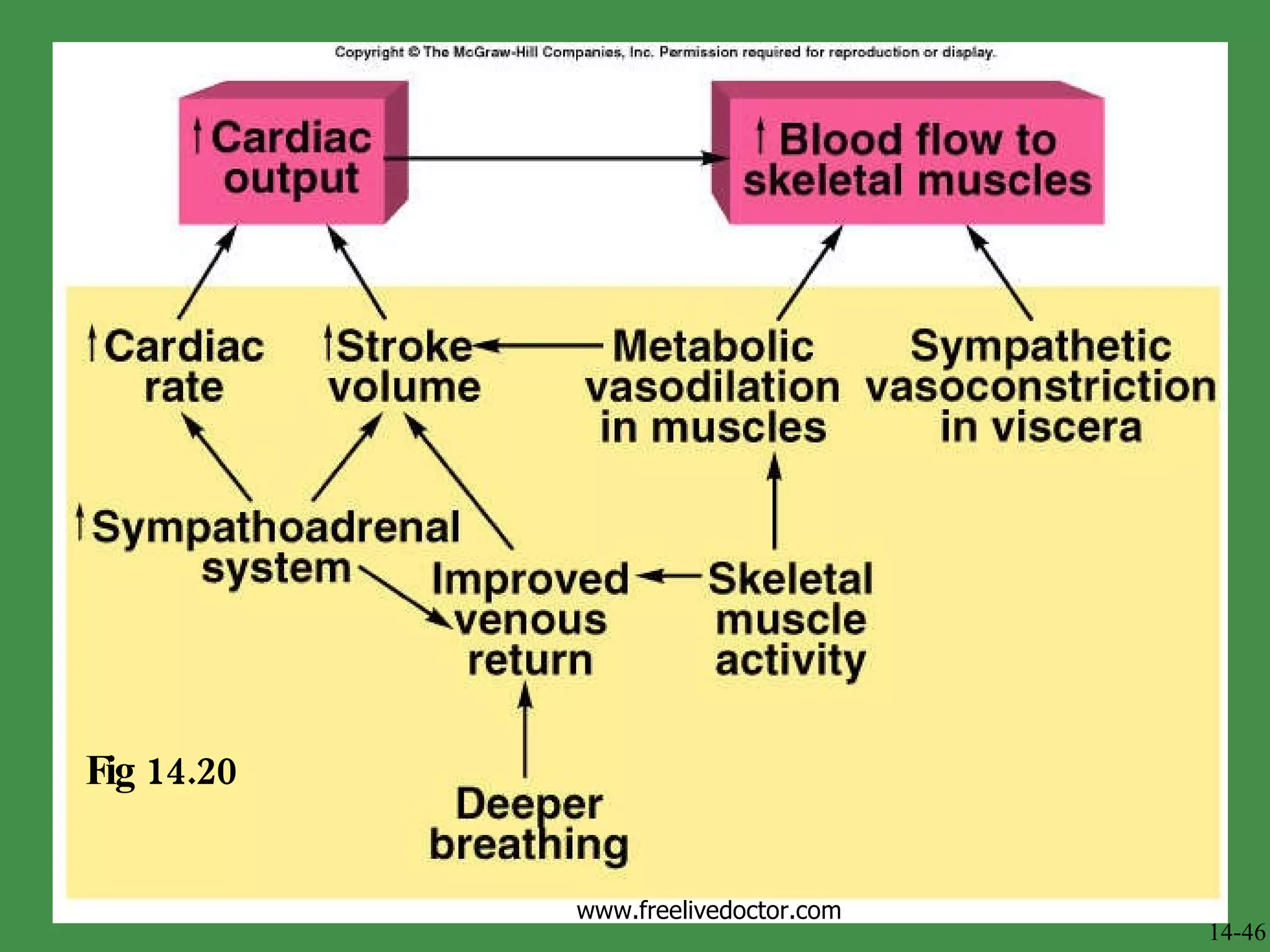
The document discusses cardiac output, blood flow, blood pressure, and factors that regulate them. It defines cardiac output as the volume of blood pumped by the heart per minute, and describes how it is determined by heart rate and stroke volume. Stroke volume depends on preload, contractility, and afterload. The autonomic nervous system and other factors control heart rate and contractility. Blood flow is determined by pressure differences and vascular resistance. The document also covers blood pressure measurement and control via the baroreceptor reflex.