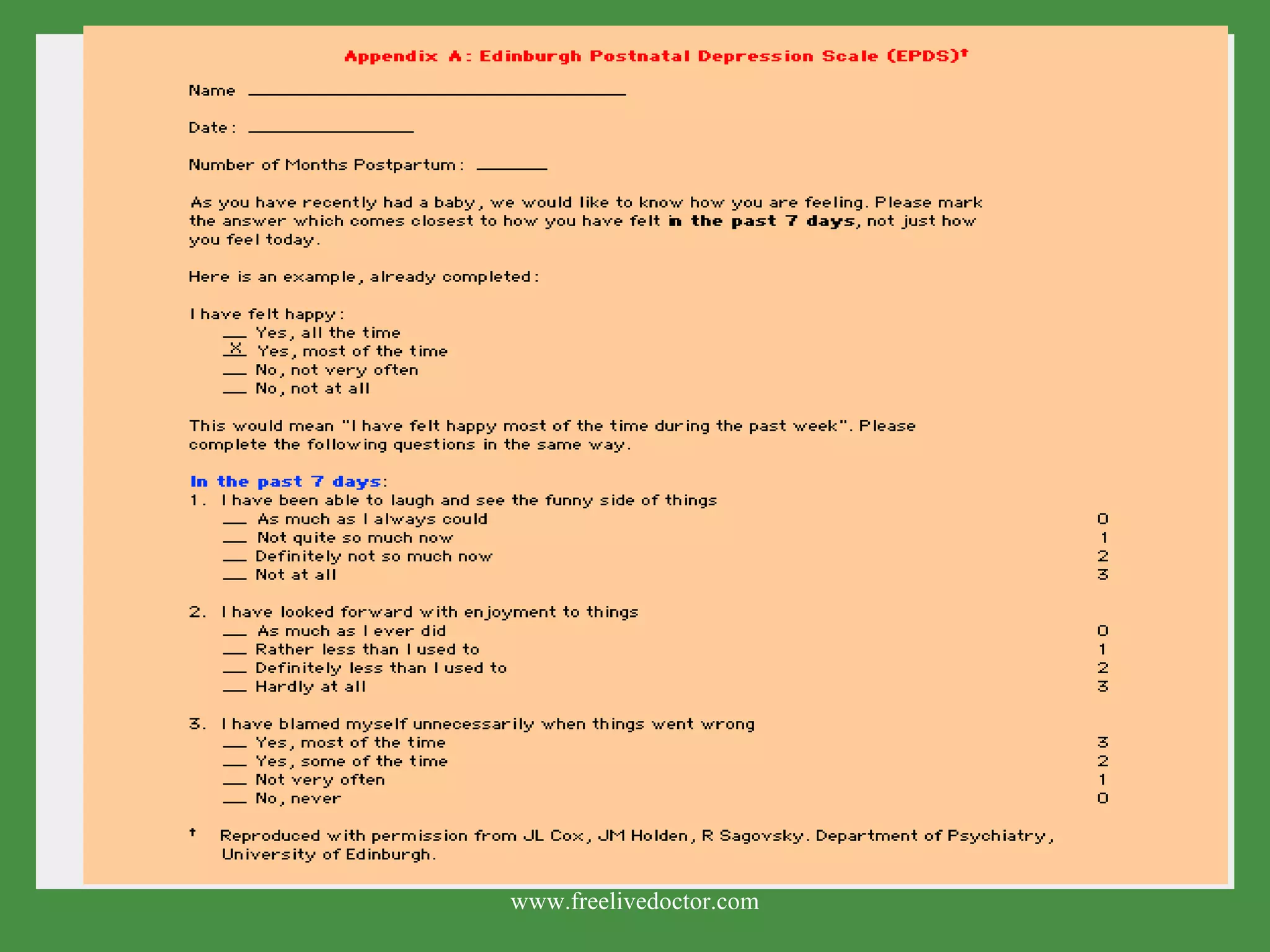
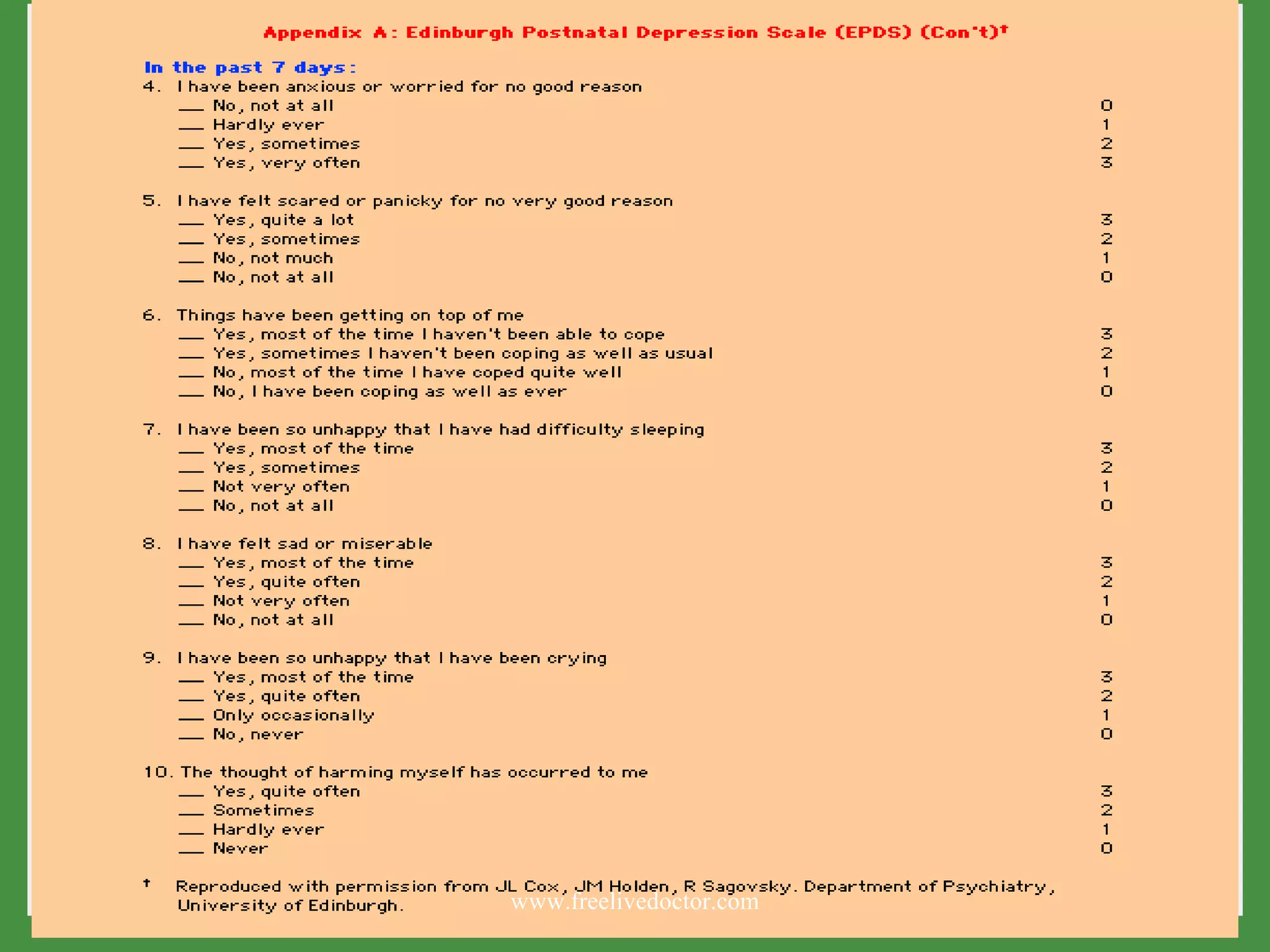
The document discusses postpartum mood disorders, including prevalence, risk factors, screening tools, diagnosis, and treatment options. It notes that postpartum mood disorders range from mild and temporary postpartum blues to more severe postpartum depression and postpartum psychosis. Screening tools like the Edinburgh Postnatal Depression Scale can help identify at-risk women. Treatment involves psychosocial therapies and may include antidepressant medication depending on severity. A multidisciplinary approach is important to address biological, psychological and social factors.


































































![Post Partum Disorders [2001]](https://cdn.slidesharecdn.com/ss_thumbnails/postpartum-170814005829-thumbnail.jpg?width=640&height=640&fit=bounds)




























