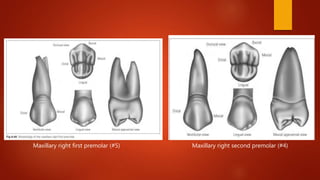
The document provides information about the permanent posterior teeth, specifically the maxillary and mandibular premolars. It defines key anatomical terms and describes the identifying features, eruption timing, root morphology, occlusion relationships, and clinical considerations of each individual premolar tooth. The maxillary and mandibular first premolars generally have two cusps and one or two roots, while the mandibular second premolar uniquely has three cusps. The document emphasizes how the premolar teeth assist in grinding food through their interdigitation with antagonists in the opposing jaw.