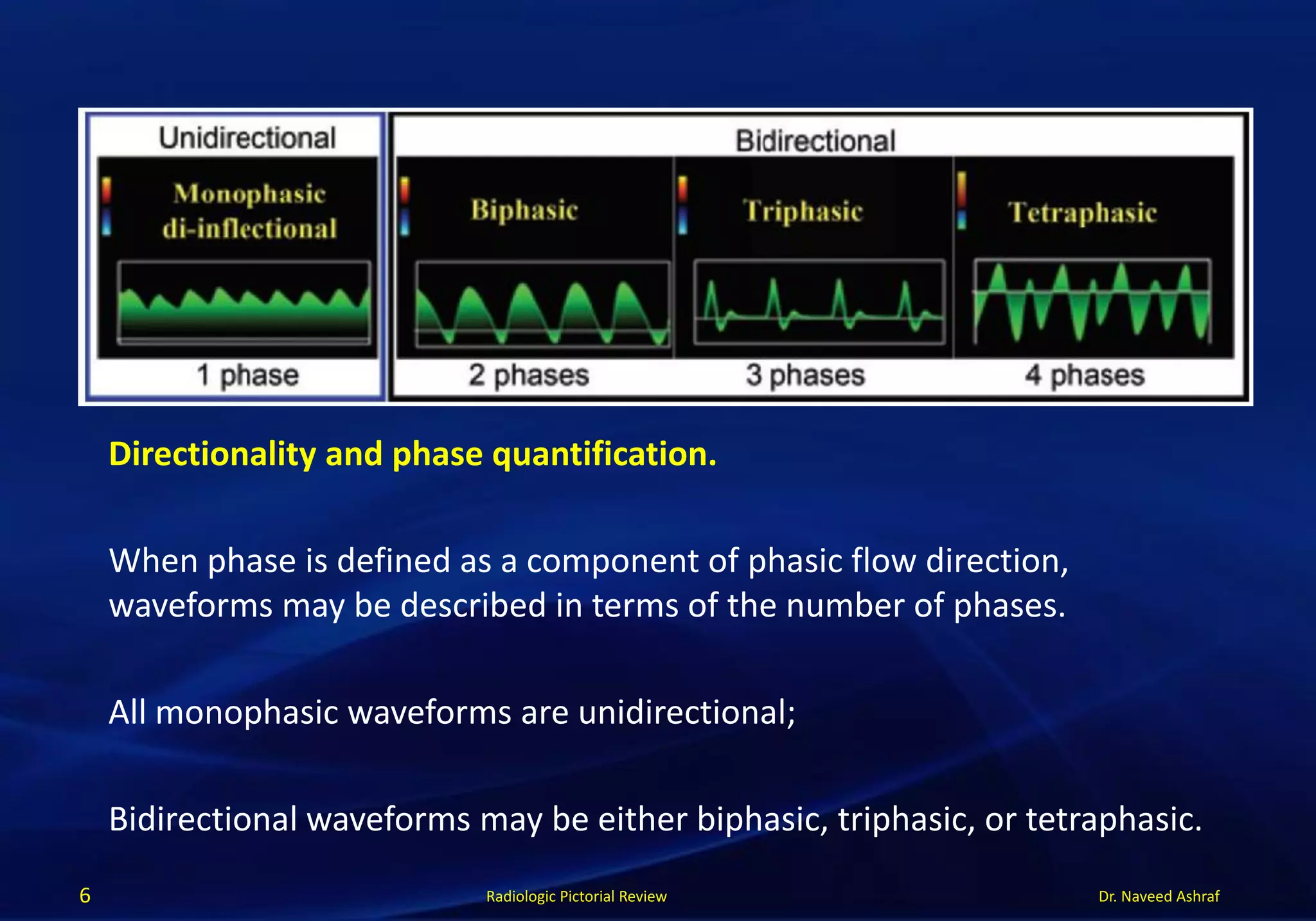
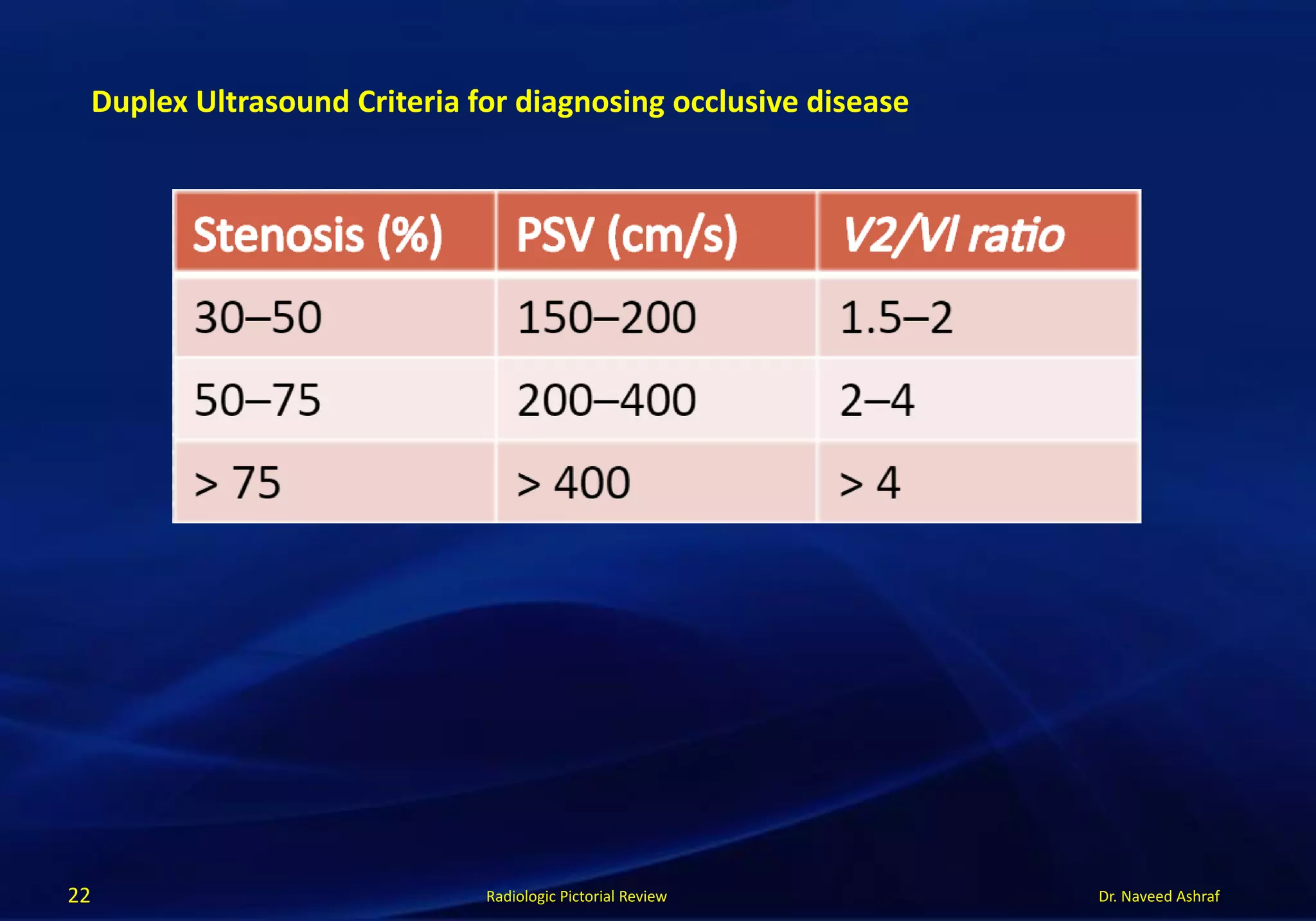
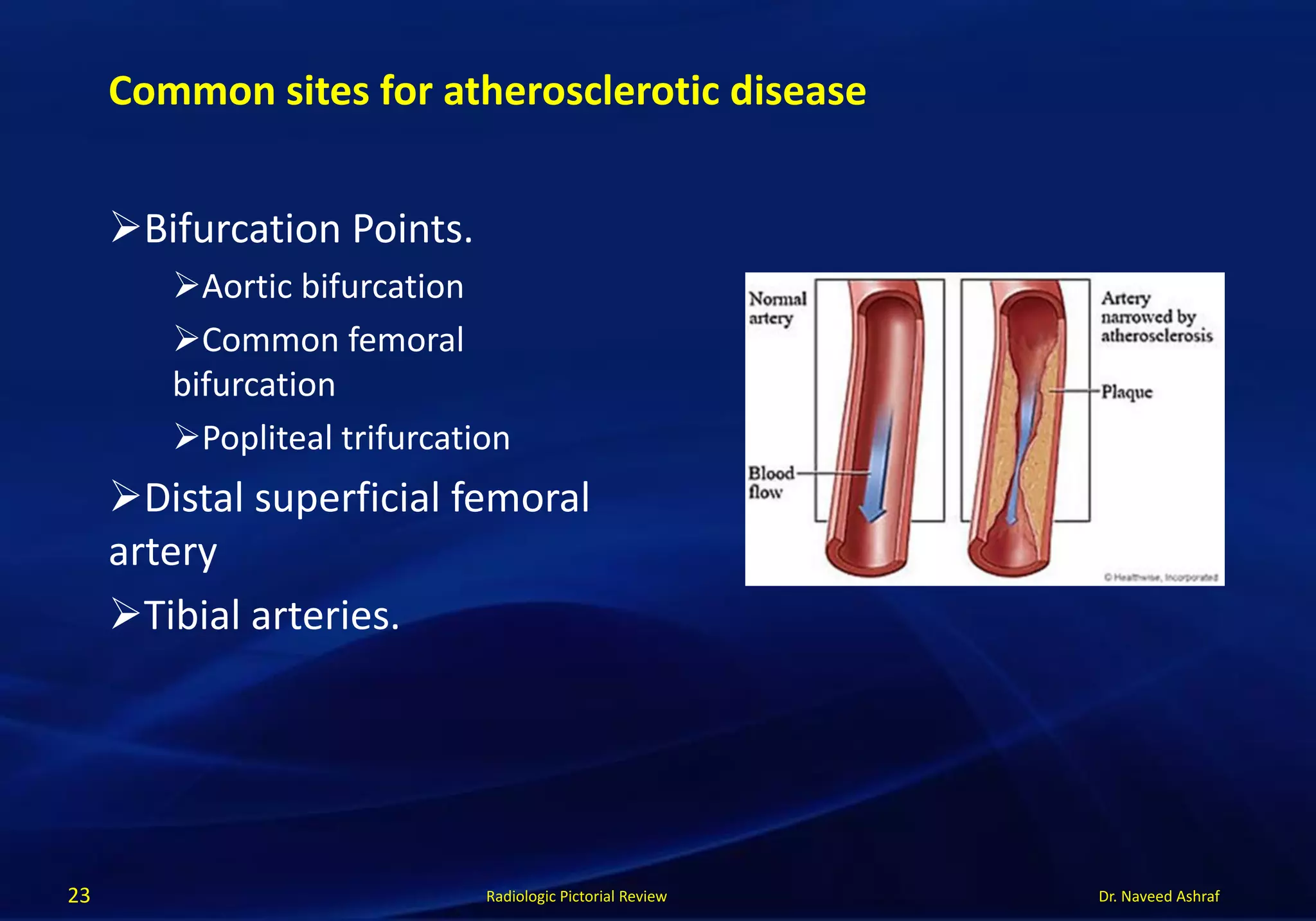
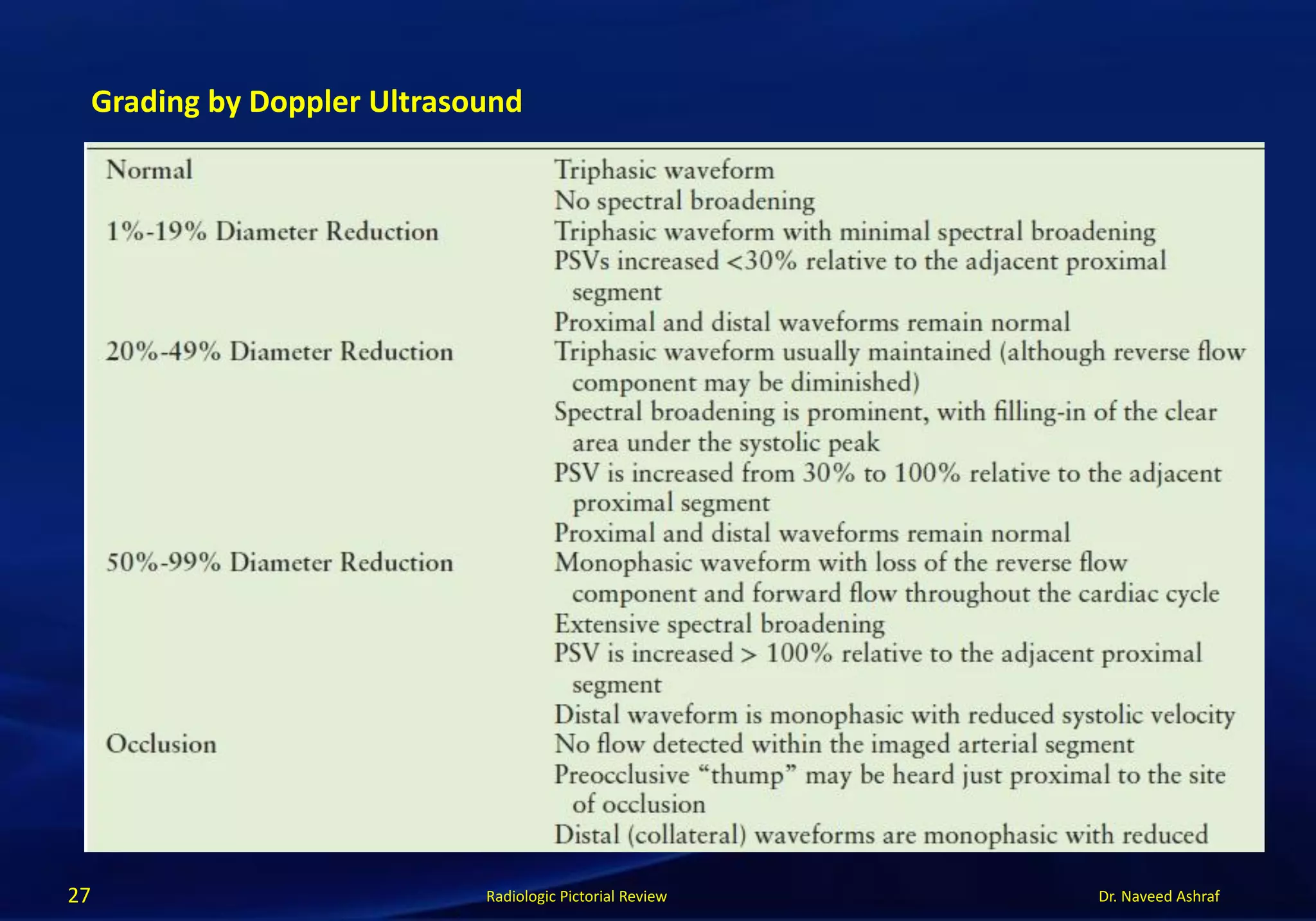
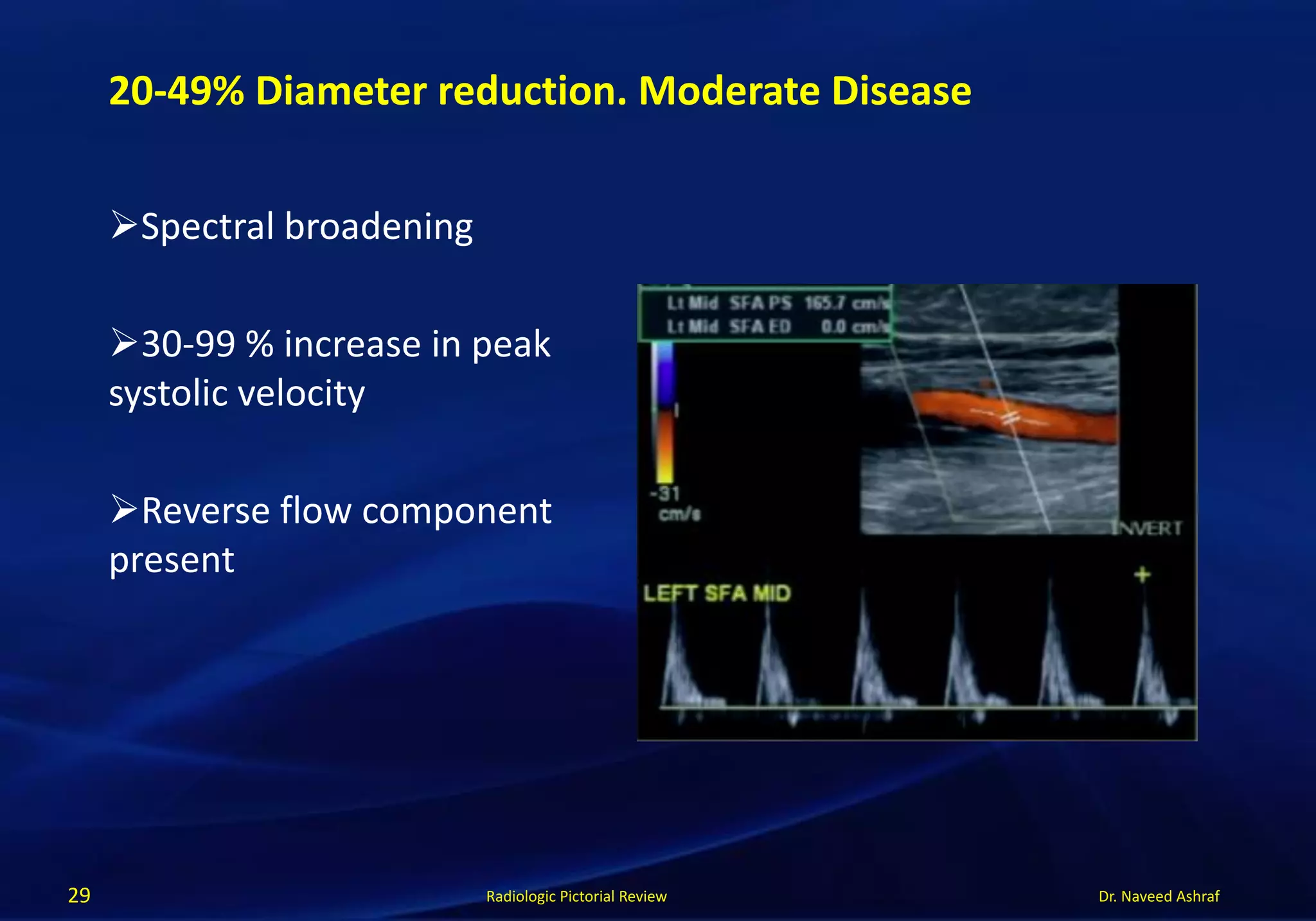
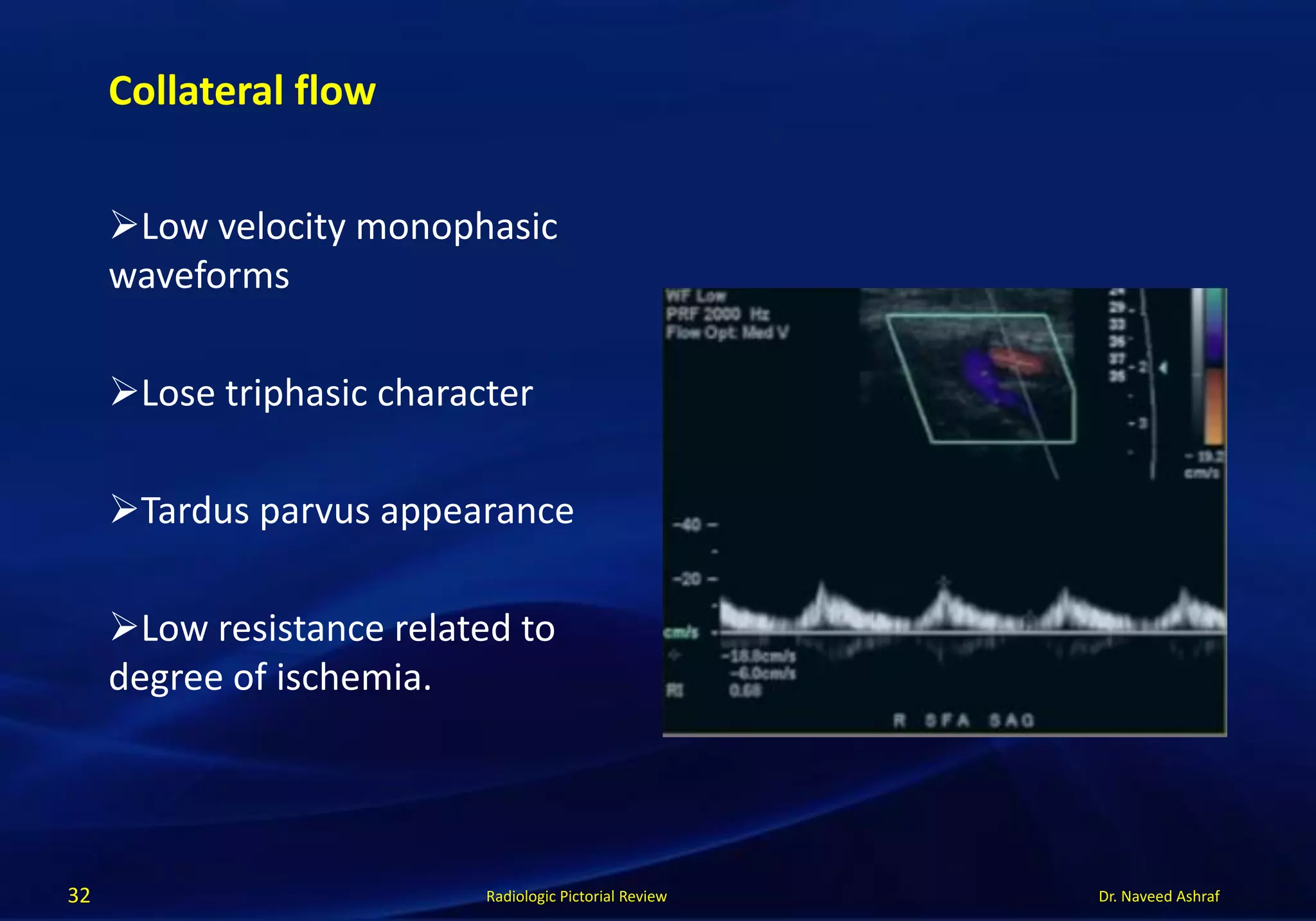
This document discusses Doppler ultrasound in peripheral arterial disease. It begins by explaining Doppler ultrasound waveforms and how they relate to blood flow direction and velocity. It then covers topics like antegrade versus retrograde flow, pulsatile versus nonpulsatile flow, and directionality. The document also discusses spectral broadening and differentiating high- versus low-resistance arteries. It provides diagrams to illustrate topics like stenosis, collateral flow, and the definitions of upstream and downstream. Finally, it outlines the criteria for classifying and grading peripheral arterial stenosis using Doppler ultrasound.