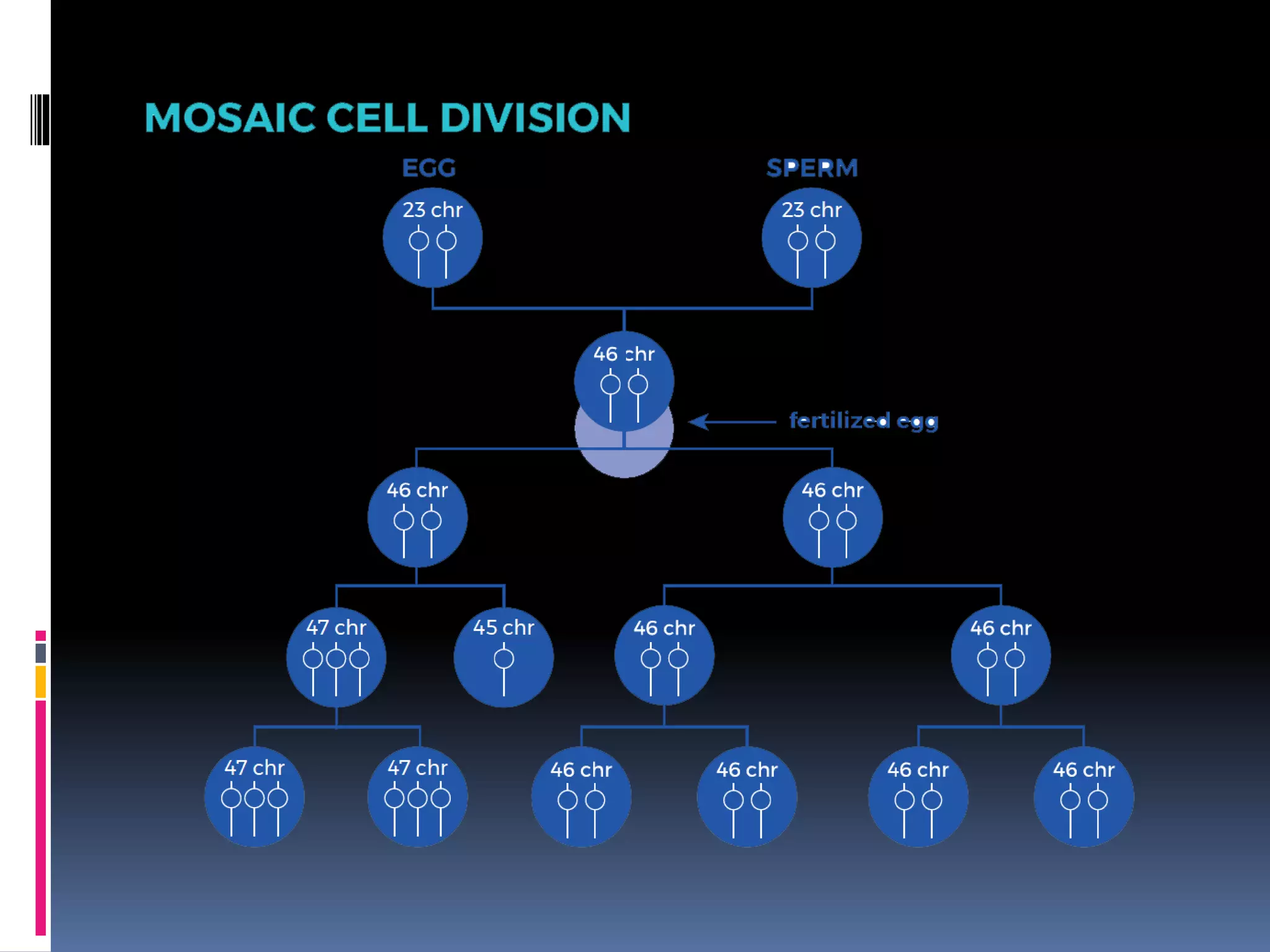
Down syndrome, caused by an extra chromosome 21, is the most common chromosomal abnormality with an estimated incidence of 0.1% in live births, leading to various health issues and intellectual disabilities. The condition can manifest in three forms: standard trisomy 21, translocations, and mosaicism, with management necessitating a multidisciplinary approach including genetic counseling, early screening, and targeted therapies. Clinical features range from physical abnormalities and vision issues to higher risks of neurological disorders, emphasizing the importance of early intervention and tailored educational strategies.