Download to read offline
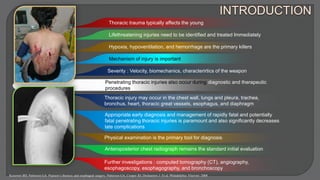


Thoracic injuries can involve the chest wall, lungs, heart, great vessels, trachea, esophagus, and diaphragm. Penetrating injuries require swift identification and treatment of life-threatening conditions like hypoxia and hemorrhage. Initial assessment involves primary and secondary surveys, along with chest x-rays, CT scans, and other imaging to diagnose injuries. Management depends on factors like the size and location of wounds. Large defects or injuries to organs may require emergency thoracotomy or thoracoscopy, while smaller wounds can sometimes be treated without surgery. Proper diagnosis and treatment can significantly reduce late complications from thoracic trauma.











































































