1) Chest trauma is predominantly caused by motor vehicle accidents and falls. The most common injuries are chest wall trauma and hemothorax.
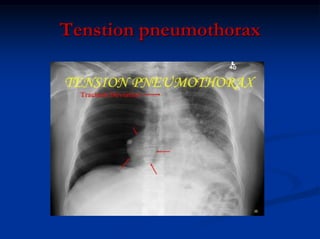
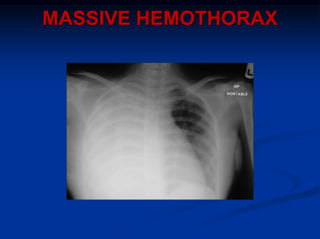
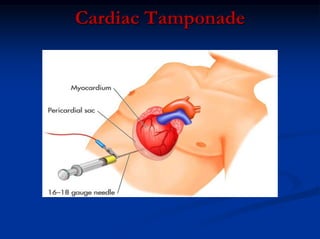
2) Early deaths from chest trauma are often caused by airway obstruction, tension pneumothorax, massive hemothorax, or cardiac tamponade.
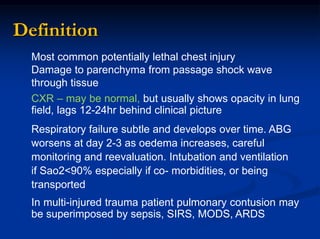
3) Initial assessment focuses on the ABCs with stabilization of life-threatening injuries like tension pneumothorax the top priority. Secondary surveys then identify and treat other injuries like simple pneumothorax, pulmonary contusion, and blunt cardiac injury.