LEARNING OUTCOMES:
• Introductionto chest trauma.
• Classification of chest trauma into deadly dozen.
• Initial evaluation and Resuscitation of Injured patient.
• Investigation and management of deadly dozen.
• Emergency thoracotomy ….Introduction , indications and contraindications, approaches.
3.
DEFINITION:
Injury to anypart of chest as a result of energy transfer from an
inflicting source that could be blunt or penetrating.
4.
INTRODUCTION:
• Chest traumaaccounts for 25% of all severe injuries.
• In a further 25% it may be significant contributor to the subsequent death of the patient.
• Approximately 80% of the patients of chest trauma can be managed non operatively.
• The key to a good outcome is Early physiological resuscitation followed by a correct
diagnosis.
INVESTIGATIONS:
• Chest Radiography
•Ultrasound/ extended Focused assessment with sonography for trauma (e FAST)
• Finger thoracostomy ( in physiologically grossly unstable patients where physical
examination is inconclusive and there is no time for radiological investigation).
• CT scan.
7.
MANAGEMENT:
• Resuscitation ofall injuries to the chest should follow the latest advanced trauma life support(ATLS) principles.
• c : Catastrophic hemorrhage
• A: Airway
• B: Breathing
• C: Circulation
• D: Disability ( NEUROLOGY)
• E: Environment and Exposure
Routine investigation in the emergency department of chest injury is based on clinical examination supplemented
by appropriate imaging.
AIRWAY OBSTRUCTION:
• Clearthe airway by suctioning of secretions or blood.
• Chin lift
• Jaw thrust
• Insertion of oropharyngeal airway
• Endotracheal intubation
10.
TENSION PNEUMOTHORAX:
• Mostcommon causes are penetrating chest trauma.
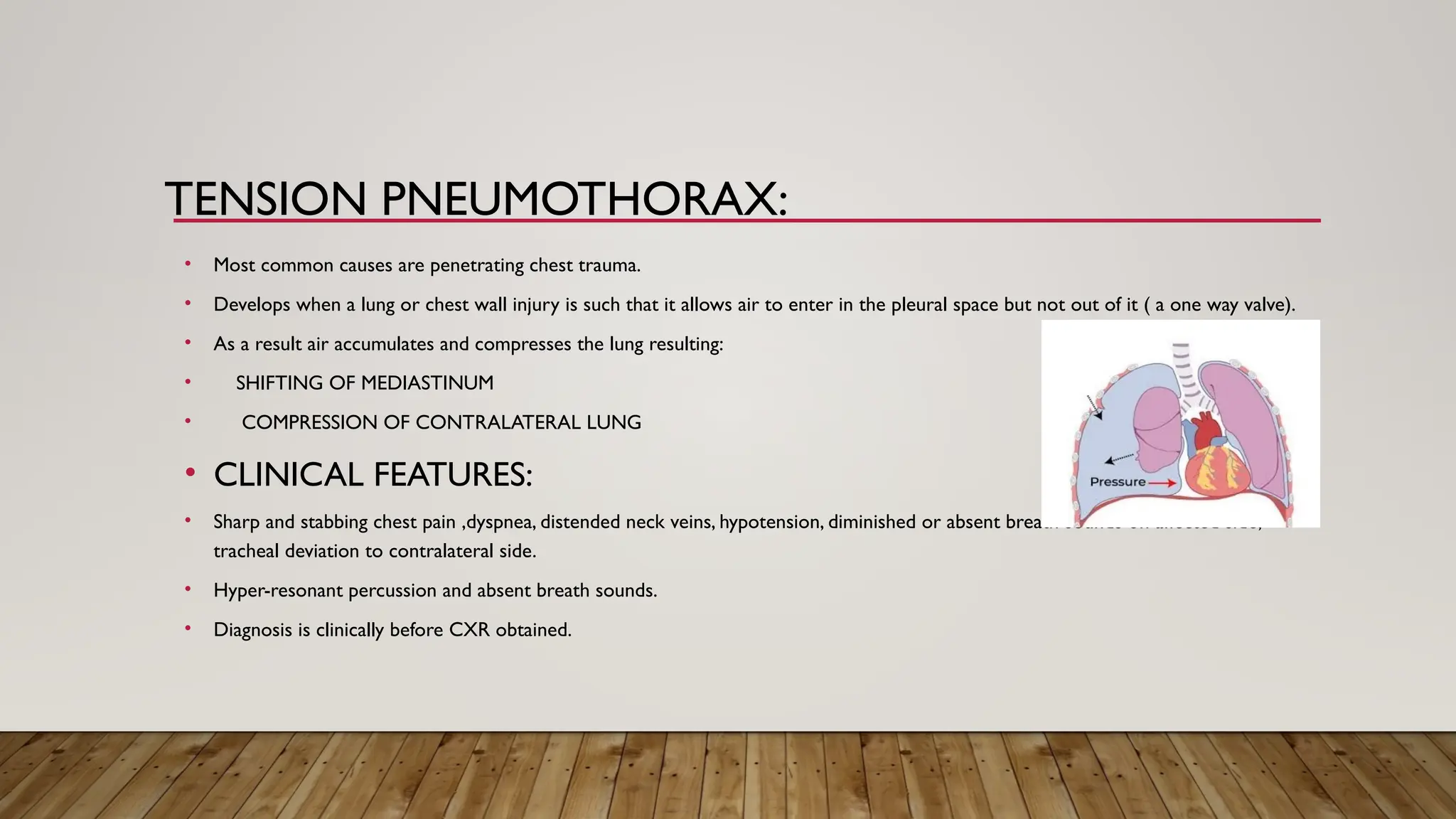
• Develops when a lung or chest wall injury is such that it allows air to enter in the pleural space but not out of it ( a one way valve).
• As a result air accumulates and compresses the lung resulting:
• SHIFTING OF MEDIASTINUM
• COMPRESSION OF CONTRALATERAL LUNG
• CLINICAL FEATURES:
• Sharp and stabbing chest pain ,dyspnea, distended neck veins, hypotension, diminished or absent breath sounds on affected side,
tracheal deviation to contralateral side.
• Hyper-resonant percussion and absent breath sounds.
• Diagnosis is clinically before CXR obtained.
INTERCOSTAL CHEST DRAIN:
•Intercostal chest drain is placed in triangle of safety which has following boundaries.
• Boundaries of Triangle of safety:
• Anteriorly: lateral border of pectoralis major
• Posteriorly: anterior border of latissimus dorsi
• Inferiorly: 5th
intercostal space at the level of nipple
15.
OPEN PNEUMOTHORAX: (SUCKINGCHEST
WOUND)
• More common in penetrating injuries than blunt thoracic injuries.
• It is due to large open defect in chest (>3cm), leading to equilibration between intrathoracic and
atmospheric pressure.
• CLINICAL FEATURES:
• Tachypnea, decreased respiratory movements on affected site
• Central trachea.
• Absent breath sounds on affected side.
• Hyper-resonant percussion.
16.
OPEN PNEUMOTHORAX: (SUCKINGCHEST
WOUND)
• TREATMENT:
• Closing the defect with a sterile occlusive plastic dressing
taped on three side to act as a flutter type valve
• Chest intubation remote from injury site.
17.
PERICARDIAL TAMPONADE:
• Mostcommonly caused by penetrating chest injuries.
• Accumulation of small amount of blood (50ml) in non distensible pericardial sac causing
compression of heart and obstruction of venous return and decreased filling of cardiac
chambers during diastole.
• Clinical features:
• Increased venous pressure, decreased arterial pressure
with tachycardia and muffled heart sounds. (BECK’STRIAD)
TREATMENT:
• Pericardiocentesis
• Correctimmediate treatment of tamponade is operative either via a subxiphoid window
on by open surgery ( sternotomy or left anterolateral thoracotomy).
• Pericardiocentesis has no role in treatment of tamponade secondary to myocardial injury
20.
MASSIVE HEMOTHORAX:
• Mostcommon source of massive hemothorax in blunt trauma is bleeding from torn
intercostal vessels or from internal mammary artery secondary to rib fractures.
• In penetrating injuries bleeding from variety of viscera may be involved.
• Clinical features:
• Hemorrhagic shock, flat neck veins, unilateral absence of breath sounds and dullness to
percussion.
MASSIVE HEMOTHORAX:
• TREATMENT:
•Correction of hypovolemic shock.
• Insertion of chest tube.
• Urgent Thoracotomy:
If initial blood loss more than 1500ml.
200ml/hour over 3-4 hours.
24.
FLAIL CHEST:
• Mostcommonly caused by blunt trauma.
• 3 or more consecutive ribs fracture in two or more locations.
• May also produce underlying pulmonary contusion.
• Diagnosed clinically in a patient who are not ventilated well and
with the help of paradoxical movement of segment.
• CT scan ( gold standard investigations).
25.
FLAIL CHEST:
• TREATMENT:
•Oxygen administration.
• Adequate analgesia
• Physiotherapy
• Ventilation ( for patients developing respiratory failure despite analgesia and oxygen)
• Surgery (internal fixation) in patients with severe injury or pulmonary contusion.
• Traumatic aorticrupture is a common cause of sudden death after a vehicle collision or fall
from a great height.
The most common site for tearing in traumatic aortic rupture is proximal descending
aorta near where the left subclavian artery branches off from the aorta distal to the
ligamentum arteriosum.
• Clinical features:
• No specific clinical features but it should be suspected in patients with asymmetry of upper
and lower extremity blood pressure, widened pulse pressure and chest wall contusion.
THORACIC AORTIC DISRUPTION
28.
THORACIC AORTIC DISRUPTION
•INVESTIGATIONS:
• Erect chest X-Ray (widened mediastinum)
• CT scan (confirmatory test)
• TREATMENT:
• Initial management consist of control of systolic pressure to less than 120mmHg.
• Thereafter endovascular intra-aortic stent can be placed or tear can be repaired by direct
repair or excision or grafting using a Dacron graft by thoracic and vascular surgeons.
MYOCARDIAL CONTUSION
TREATMENT:
• Conservativemanagement if hemodynamically stable.
• Inotropic support if blood pressure falling down.
• Close monitoring because of risk of cardiac arrythmias.
• Rarely require surgical intervention.
32.
DIAPHRAGMATIC INJURIES
• Anypenetrating injury below the fifth intercostal space should raise suspicion of diaphragmatic
penetration and therefore, injury to abdominal contents.
• The diaphragmatic rupture is usually large with herniation of abdominal contents into the chest.
• INVESTIGATIONS:
• Chest radiography after placement of NG tube may be helpful ( may show the stomach herniation
into the chest).
• CT Scan with contrast.
• Video assisted thoracoscopy or laparoscopy ( most accurate evaluation)
33.
DIAPHRAGMATIC INJURIES
• TREATMENT:
•Operative repair is recommended in all cases.
• All penetrating diaphragmatic injury must be repaired via the abdomen- not the chest- to
rule out penetrating hollow viscus injury.
34.
ESOPHAGEAL INJURY
• Mostesophageal injuries result from penetrating trauma.
• Esophagus has no serosal covering and any perforation results in direct drainage into mediastinum.
• The patient may present with odynophagia, subcutaneous or mediastinal emphysema, pleural
effusion, air in peri-esophageal space and unexplained fever.
• Mediastinal and deep cervical emphysema are evidence of an aerodigestive injury until proven
otherwise.
35.
ESOPHAGEAL RUPTURE:
• INVESTIGATIONS:
•CT scan with oral contrast
• Esophagoscopy with esophagogram (detect 90% of esophageal injuries)
• TREATMENT:
• Suspension of all oral intakes.
• IV antibiotics and fluids for resuscitation.
• Operative repair of any defect and drainage.
36.
PULMONARY CONTUSION
• Pulmonarycontusion occur more frequently following blunt trauma and is usually
associated with a flail segment or fractured ribs.
• This is the major cause of hypoxemia after blunt trauma.
• Hemoptysis or blood in endotracheal tube is a sign of pulmonary contusion.
PULMONARY CONTUSION
• TREATMENT:
•In mild contusion, the treatment is oxygen administration, pulmonary toilet and adequate
analgesia.
• In more severe cases, mechanical ventilation is necessary.
39.
TRACHEOBRONCHIAL INJURIES
• Almost80% of injuries in blunt trauma causes death at site or transportation to hospital.
• Severe subcutaneous emphysema with respiratory compromise can suggest
tracheobronchial disruption.
• CLINICAL FEATURES:
• Respiratory distress
• A chest drain placed on the affected side will reveal a large air leak and the collapsed lung may fail
to re-expand
EMERGENCY THORACOTOMY
• GOALSOF EDT:
• Internal cardiac massage in cardio-vascularly ‘Full’ patient. ( NO ROLE FOR INTERNAL
MASSAGE IN THE EMPTY PATIENT).
• Control of hemorrhage from injury to heart or lung.
• Control of intra-thoracic hemorrhage from other sources.
• Control of massive air leak.
• Clamping of the thoracic aorta to preserve blood supply to heart and brain.
42.
EMERGENCY THORACOTOMY
• Emergencythoracotomy should be reserved for those patients with penetrating injuries in whom signs of
life are still present.
• INDICATIONS:
• Salvageable post injury cardiac arrest:
• Patient sustaining witnessed penetrating trauma to the torso with less than 15 minutes of prehospital CPR.
• Patient sustaining witnessed blunt trauma with less than 10 minutes of prehospital CPR.
• Patient sustaining witnessed penetrating trauma to the neck or extremities with less than 5 minutes of pre
hospital CPR.
43.
EMERGENCY THORACOTOMY
• Persistentsevere post injury hypotension (SBP < 60mmHg) due to
• Cardiac tamponade
• Hemorrhage ( intrathoracic, intraabdominal, extremity, cervical)
• Air embolism
• 1500ml of blood after passing chest tube ( massive hemothorax)
• 200ml of blood/hour for 3-4 hour (massive hemothorax)
44.
CONTRAINDICATIONS
• Penetrating trauma:CPR > 15 minutes and no signs of life.
• Blunt Trauma: CPR > 10 minutes and no signs of life
• Non traumatic cardiac arrest
• Penetrating trauma without cardiac activity
• Severe head and multi system injuries
• Improperly trained team.
• Insufficient equipment
• Old age > 55 years
45.
APPROACHES OFTHORACOTOMY
• Leftanterolateral thoracotomy
• Left lung and left hilum
• Thoracic aorta
• Origin of left subclavian artery
• Left side of heart
• Lower esophagus
46.
APPROACHES OFTHORACOTOMY
• RightanterolateralThoracotomy
• Right lung and hilum
• Azygos vein
• Superior vena cava
• Infracardiac inferior vena cava
• Upper esophagus
• Thoracic aorta
47.
APPROACHES OFTHORACOTOMY:
• Mediansternotomy:
• Anterior aspect of heart
• Ascending aorta and arch of aorta
• Pulmonary arteries
• Carina of trachea