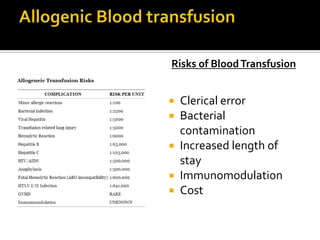
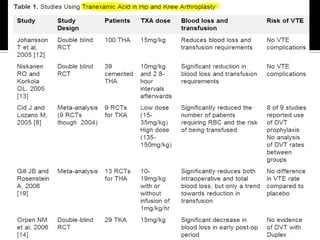
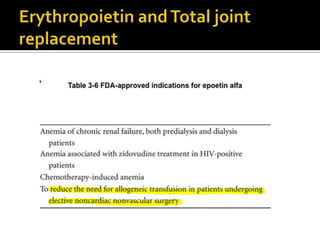
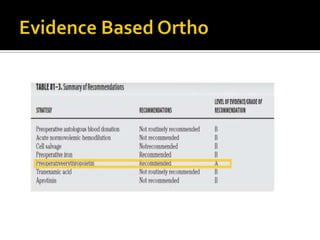
The document discusses strategies to reduce blood loss and transfusion requirements during total hip and knee replacement surgeries. It notes that average blood loss is 1.5 liters for THR and TKR but hidden blood loss accounts for 26-50% more. Revision surgeries have even higher blood loss. Options discussed to reduce transfusions include preoperative autologous blood donation, blood conservation measures, use of erythropoietin to increase hematocrit levels preoperatively, and hemostatic agents. Risks of transfusions include errors, infections, increased costs and length of stay.