Downloaded 509 times
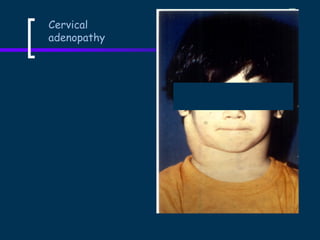
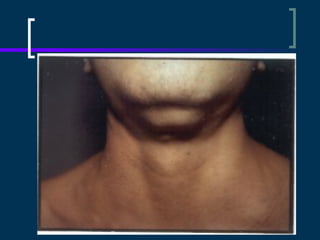
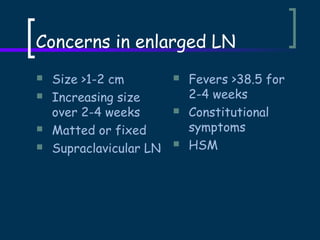
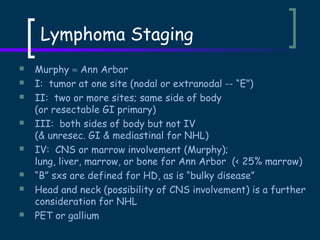
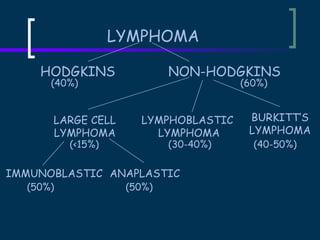
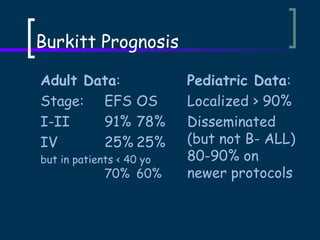


This document provides an overview of pediatric lymphomas. It discusses cervical adenopathy concerns, indications for biopsy, staging evaluations, lymphoma classifications including Hodgkin's disease and non-Hodgkin's lymphomas, clinical presentations, treatment approaches, and prognostic factors. Key points covered include types of non-Hodgkin's lymphoma, characteristics of Burkitt's lymphoma, signs of Hodgkin's disease, and treatment dependent on age, stage and tumor burden.























































































