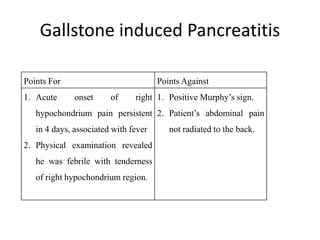


1. A 50-year-old man presented with 4 days of right upper abdominal pain, low-grade fever, and tea-colored urine. 2. Physical examination revealed tenderness in the right hypochondrium region and a positive Murphy's sign. Ultrasound showed thickened gallbladder walls, pericholecystic collection, and gallstones. 3. He was diagnosed with acute cholecystitis secondary to cholelithiasis. As medical management failed to provide relief, laparoscopic cholecystectomy was recommended to definitively treat his condition and prevent future complications or recurrence of stones.