Introduction
Hematuria means bloodin urine.
It may be Gross or macroscopic and microscopic
hematuria
Gross hematuria is seen by naked eyes while
microscopic hematuria needs microscope.
Hematuria is defined as the presence of at
least 5 red blood cells per HPF of centrifuged
urine and/or 5 RBC per microliter in
uncentrifuged specimen
4.
• Pathophysiology:
Structural disruption in the integrity of
glomerular basement membrane caused by
inflammatory or immunologic processes
Toxic disruptions of the renal tubules
Mechanical erosion of mucosal surfaces in
the genitourinary tract
History:
• Age: 2-5yrs: Wilms tumor
5-12yrs: PSGN
• Sex: F>>M in >1-2yrs: UTI
F>>M: SLE nephritis
M>F : X-linked form of Alport syndrome
• Race: whites: Idiopathic hypercalciuria
blacks: Sickle cell disease
13.
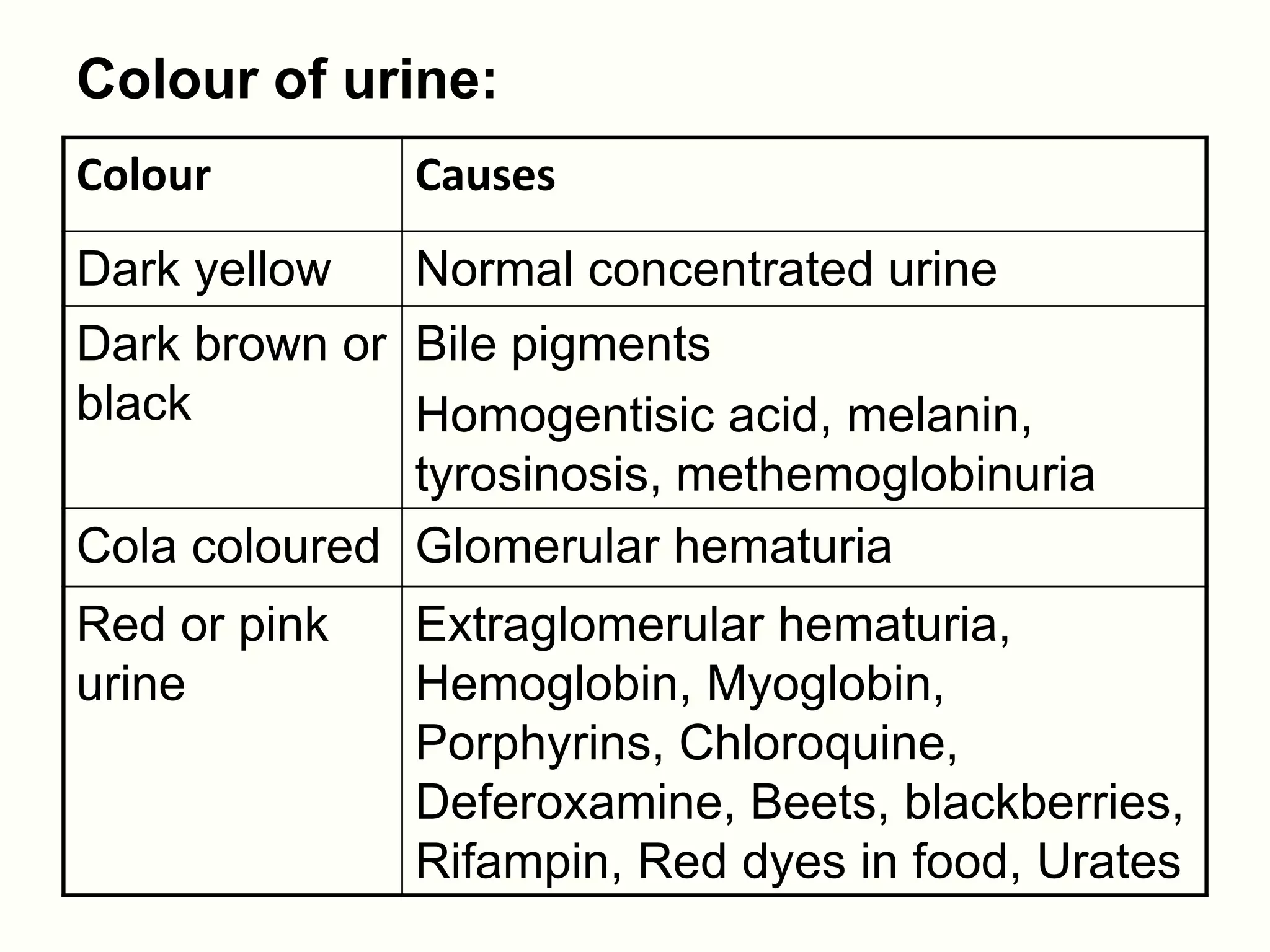
Colour of urine:
Colour Causes
Dark yellow Normal concentrated urine
Dark brown or Bile pigments
black Homogentisic acid, melanin,
tyrosinosis, methemoglobinuria
Cola coloured Glomerular hematuria
Red or pink Extraglomerular hematuria,
urine Hemoglobin, Myoglobin,
Porphyrins, Chloroquine,
Deferoxamine, Beets, blackberries,
Rifampin, Red dyes in food, Urates
14.
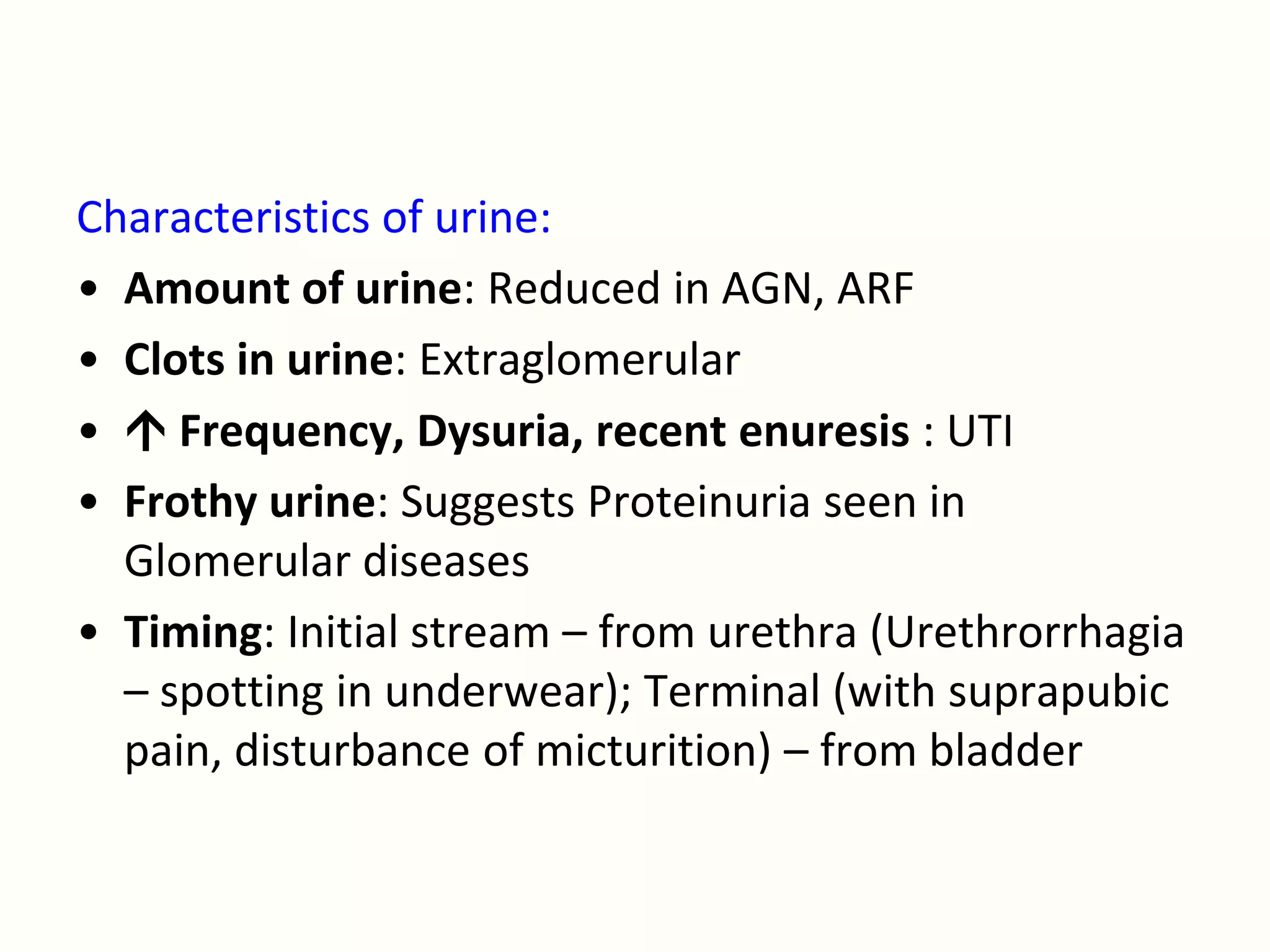
Characteristics of urine:
•Amount of urine: Reduced in AGN, ARF
• Clots in urine: Extraglomerular
• Frequency, Dysuria, recent enuresis : UTI
• Frothy urine: Suggests Proteinuria seen in
Glomerular diseases
• Timing: Initial stream – from urethra (Urethrorrhagia
– spotting in underwear); Terminal (with suprapubic
pain, disturbance of micturition) – from bladder
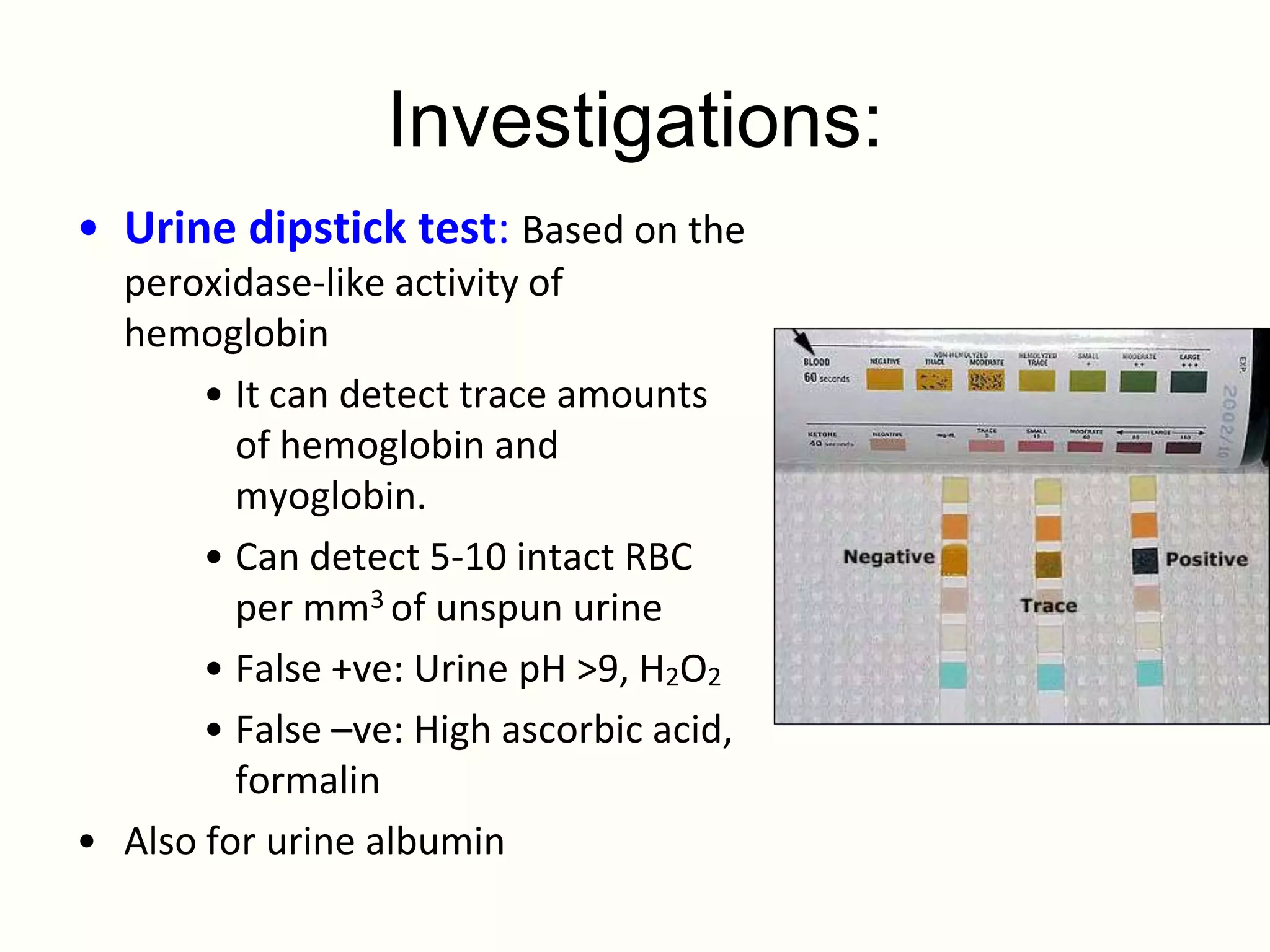
Investigations:
• Urine dipsticktest: Based on the
peroxidase-like activity of
hemoglobin
• It can detect trace amounts
of hemoglobin and
myoglobin.
• Can detect 5-10 intact RBC
per mm3 of unspun urine
• False +ve: Urine pH >9, H2O2
• False –ve: High ascorbic acid,
formalin
• Also for urine albumin
22.
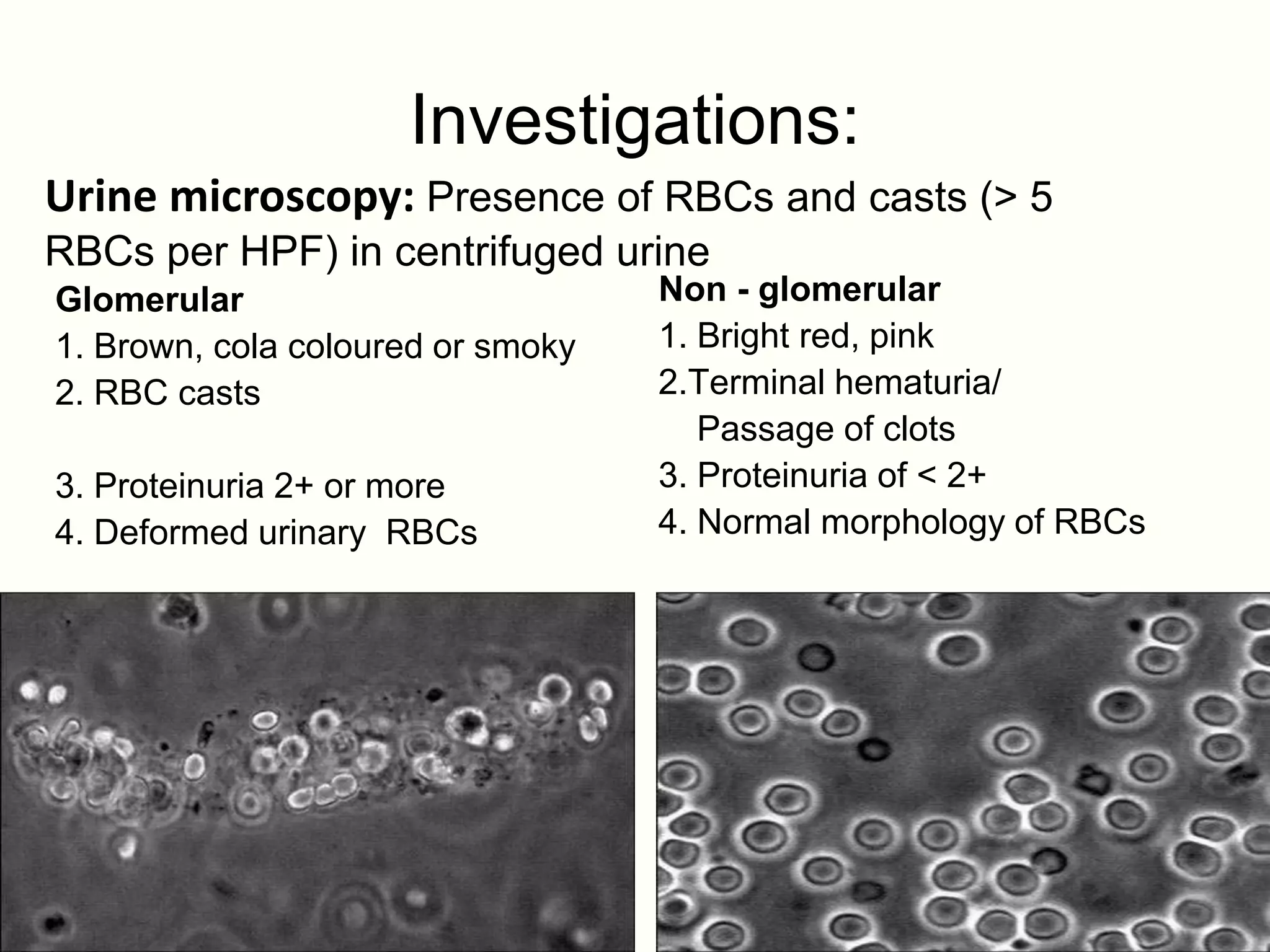
Investigations:
Urine microscopy: Presenceof RBCs and casts (> 5
RBCs per HPF) in centrifuged urine
Glomerular Non - glomerular
1. Brown, cola coloured or smoky 1. Bright red, pink
2. RBC casts 2.Terminal hematuria/
Passage of clots
3. Proteinuria 2+ or more 3. Proteinuria of < 2+
4. Deformed urinary RBCs 4. Normal morphology of RBCs
23.
Study on Evaluationof hematuria using the urinary albumin-
to-total-protein ratio to differentiate glomerular and
nonglomerular bleeding
•N. Ohisa · R. Matsuki · H. Suzuki · H. Miura · Y. Ohisa · K. Yoshida
Department of Clinical Laboratory, Tohoku University Hospital,
Sendai, Japan
•microscopy-based differentiation is not only tedious but the sensitivity and
specificity may vary from one examiner to another. Furthermore, once
the specimen has been frozen, differentiation becomes difficult.
•A total of 143 random urine specimens from patients seen at the Division of
Nephrology, Endocrinology and Vascular Disease and the Urology Department
at Tohoku University Hospital were included in the study. The inclusion criterion
for the study was a diagnosis of glomerular disease based on clinical features
or histopathology with hematuria (5 or more RBCs per high-power fi eld). Of the
104 patients diagnosed with glomerular disease and 39 specimens from
patients with nonglomerular disease, used as controls in the study.
24.
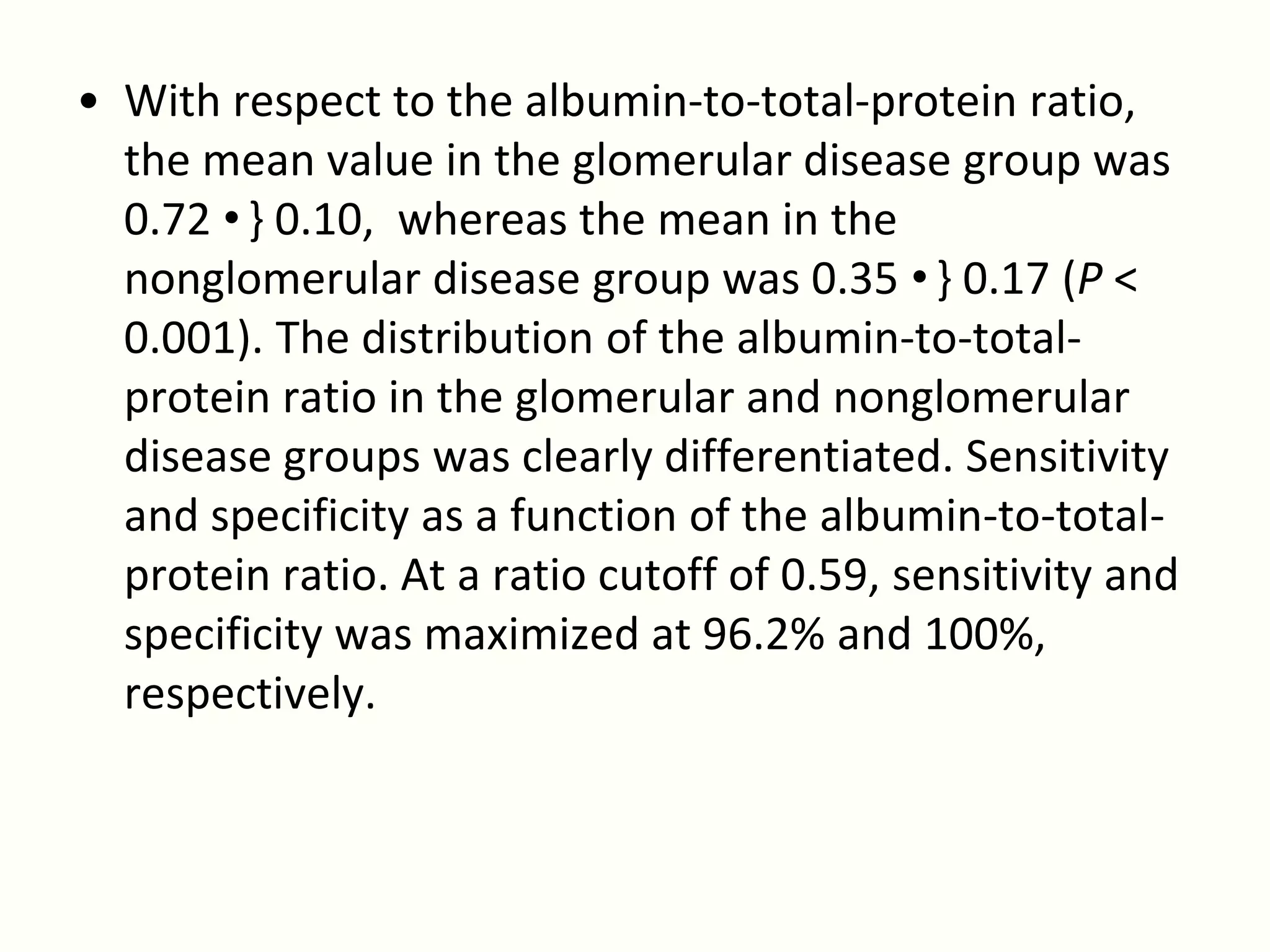
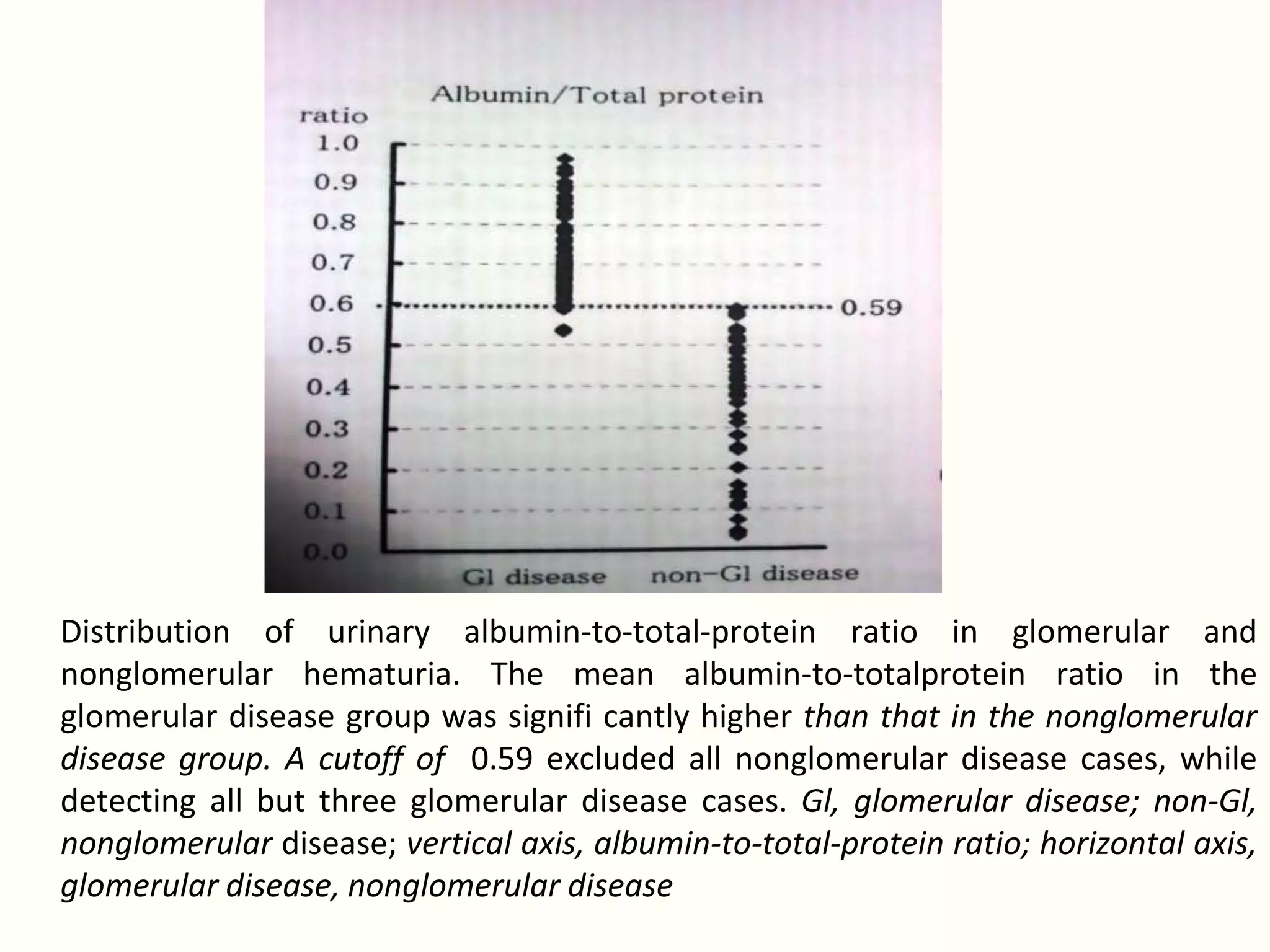
• With respectto the albumin-to-total-protein ratio,
the mean value in the glomerular disease group was
0.72 •} 0.10, whereas the mean in the
nonglomerular disease group was 0.35 •} 0.17 (P <
0.001). The distribution of the albumin-to-total-
protein ratio in the glomerular and nonglomerular
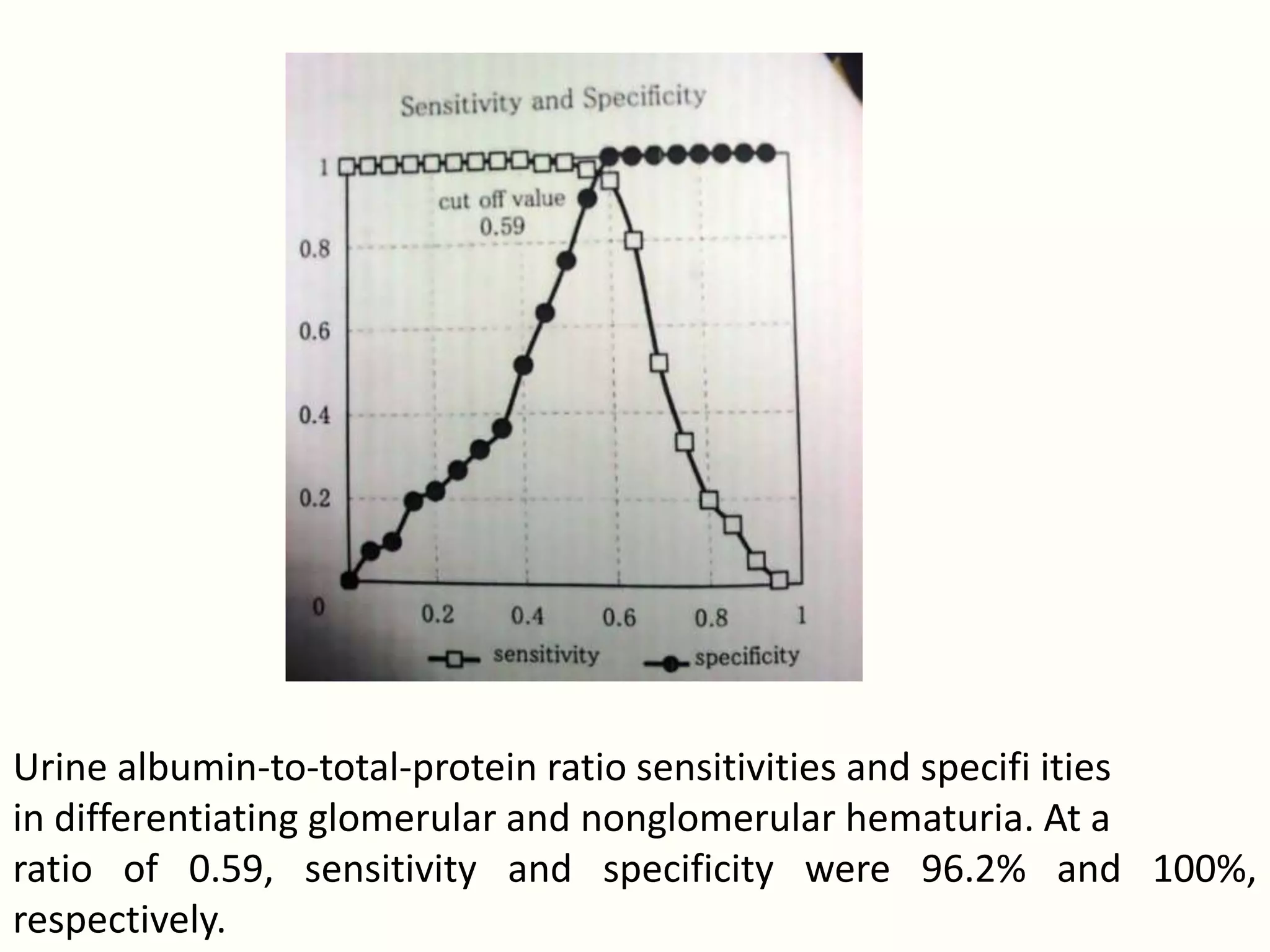
disease groups was clearly differentiated. Sensitivity
and specificity as a function of the albumin-to-total-
protein ratio. At a ratio cutoff of 0.59, sensitivity and
specificity was maximized at 96.2% and 100%,
respectively.
25.
Distribution of urinaryalbumin-to-total-protein ratio in glomerular and
nonglomerular hematuria. The mean albumin-to-totalprotein ratio in the
glomerular disease group was signifi cantly higher than that in the nonglomerular
disease group. A cutoff of 0.59 excluded all nonglomerular disease cases, while
detecting all but three glomerular disease cases. Gl, glomerular disease; non-Gl,
nonglomerular disease; vertical axis, albumin-to-total-protein ratio; horizontal axis,
glomerular disease, nonglomerular disease
26.
Urine albumin-to-total-protein ratiosensitivities and specifi ities
in differentiating glomerular and nonglomerular hematuria. At a
ratio of 0.59, sensitivity and specificity were 96.2% and 100%,
respectively.
27.
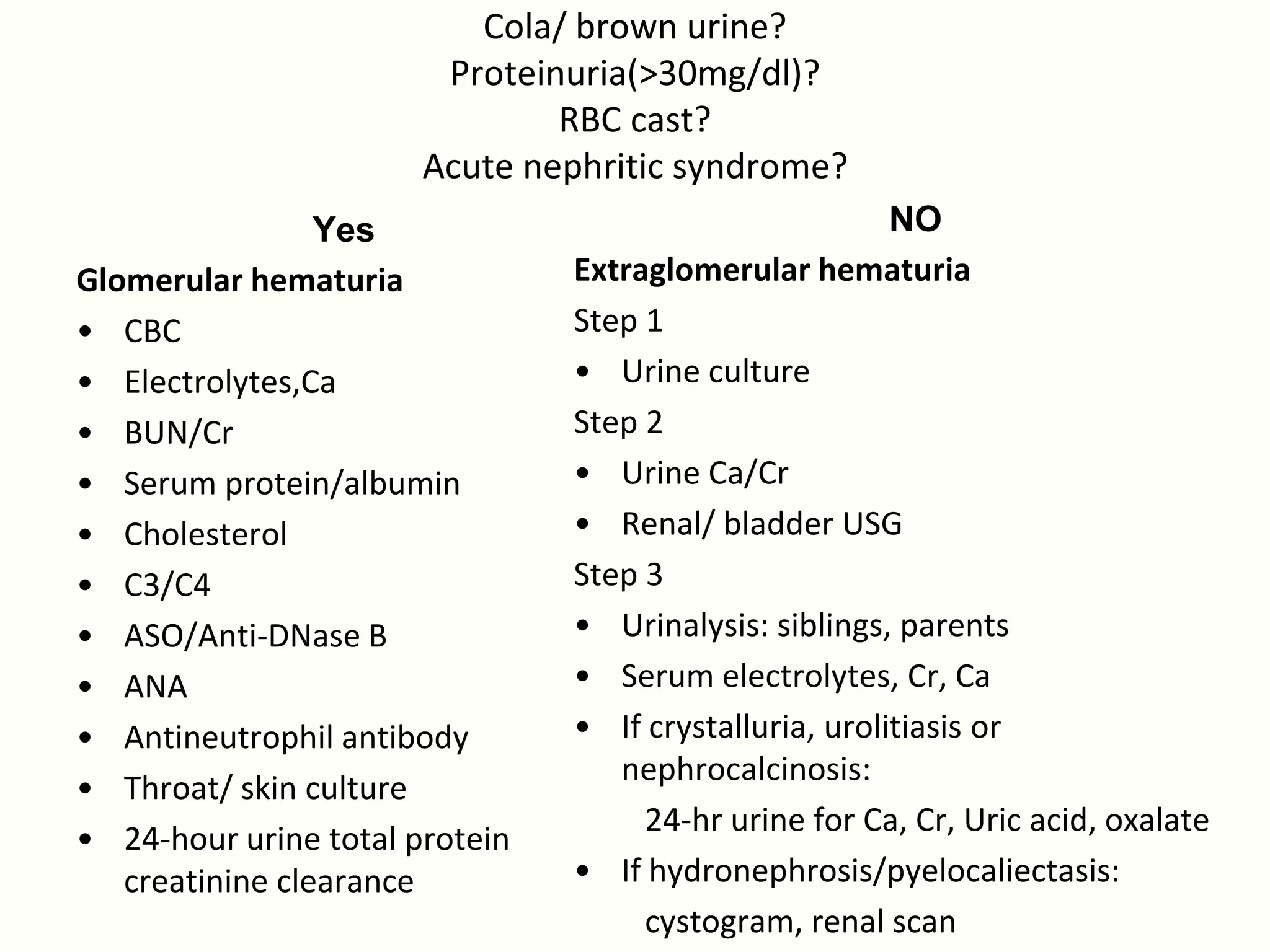
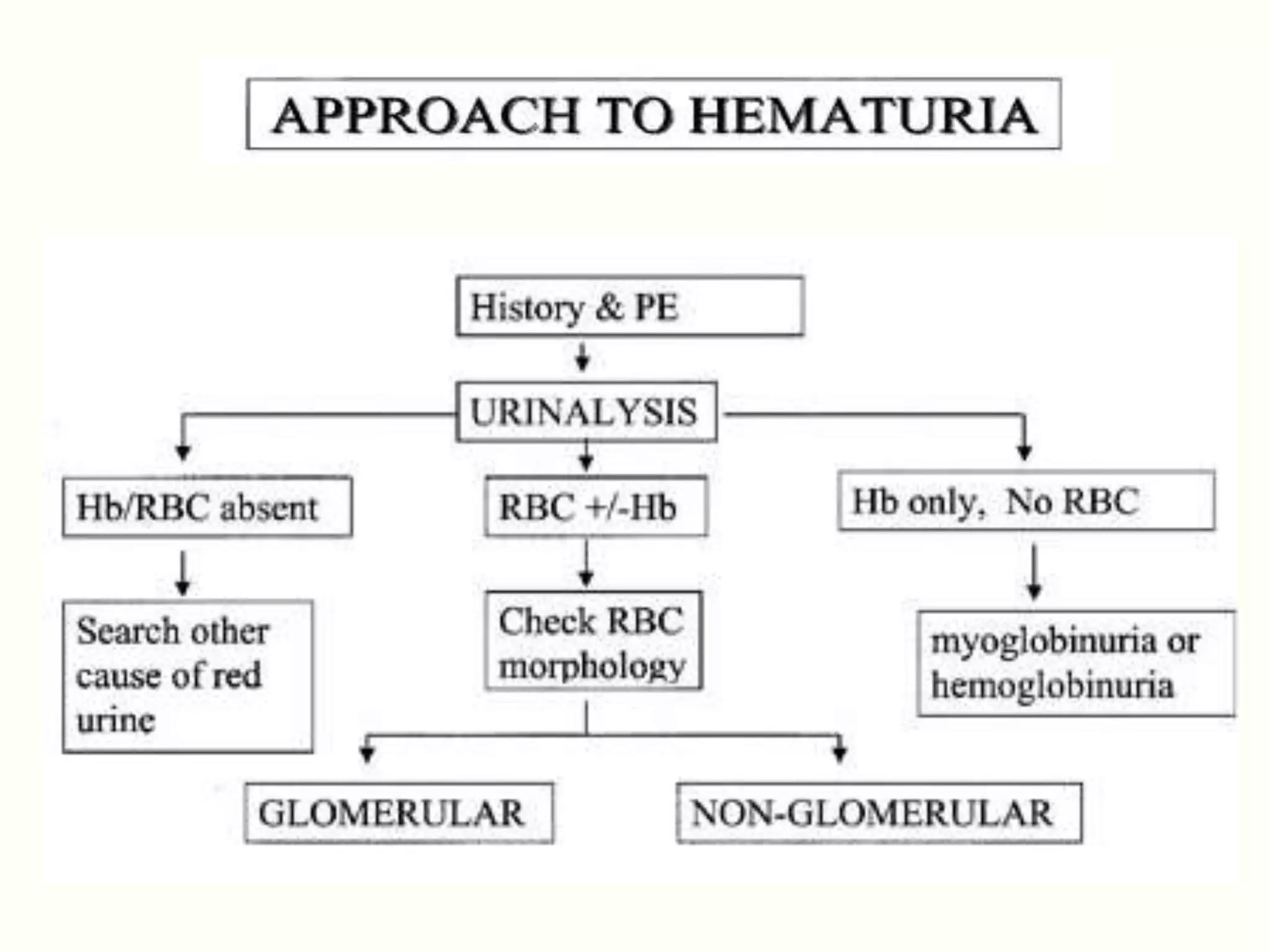
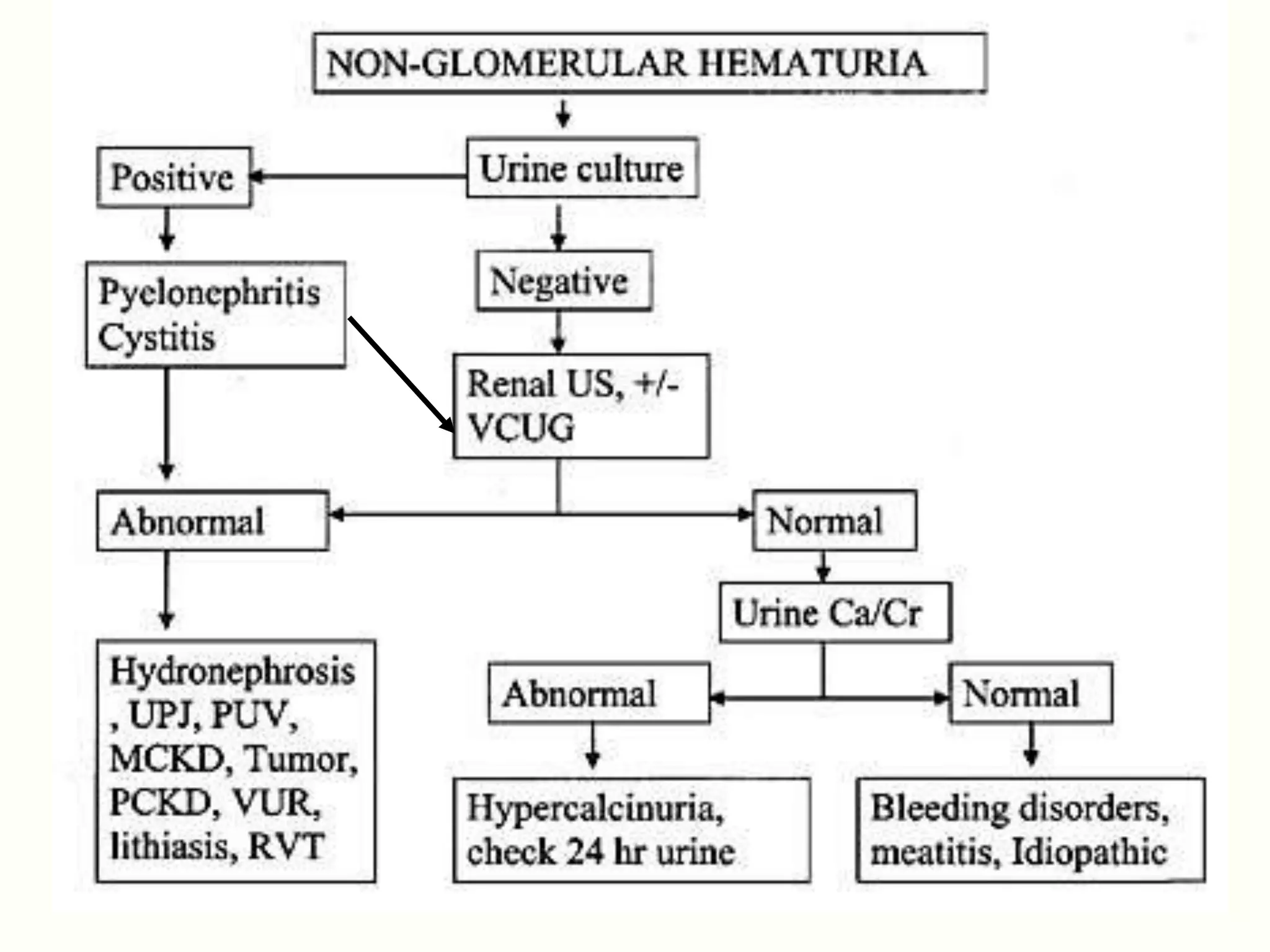
Cola/ brown urine?
Proteinuria(>30mg/dl)?
RBC cast?
Acute nephritic syndrome?
Yes NO
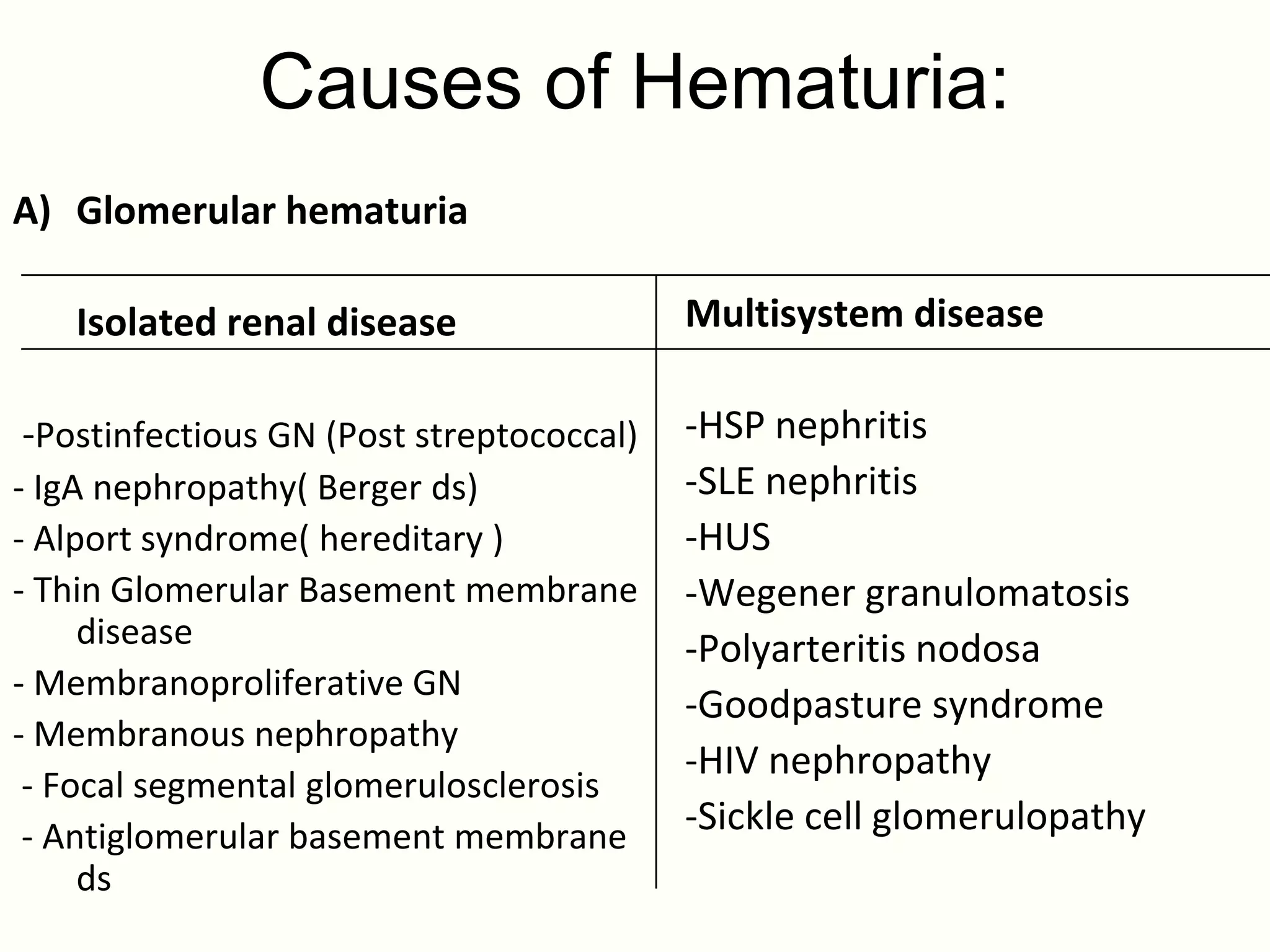
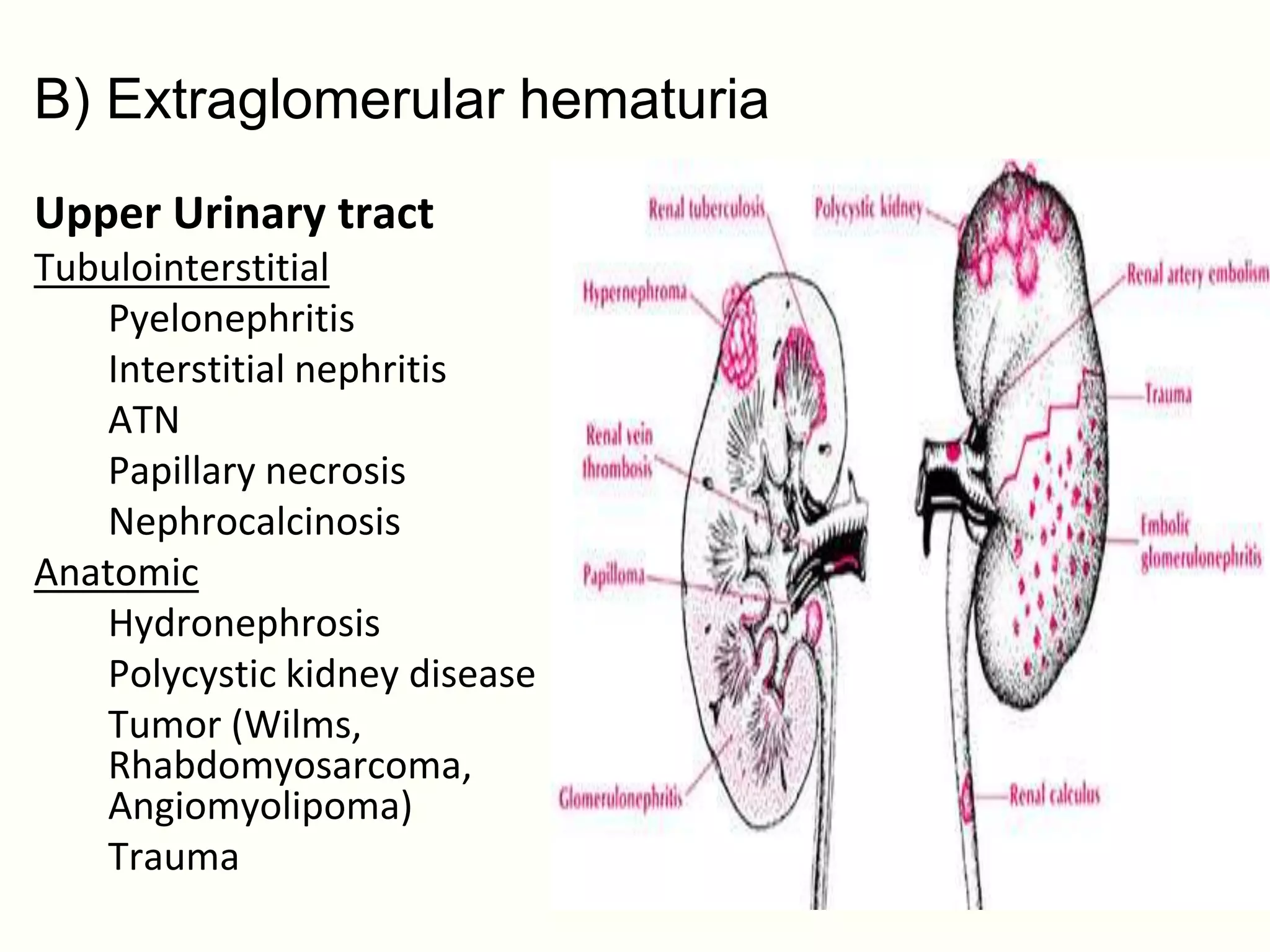
Glomerular hematuria Extraglomerular hematuria
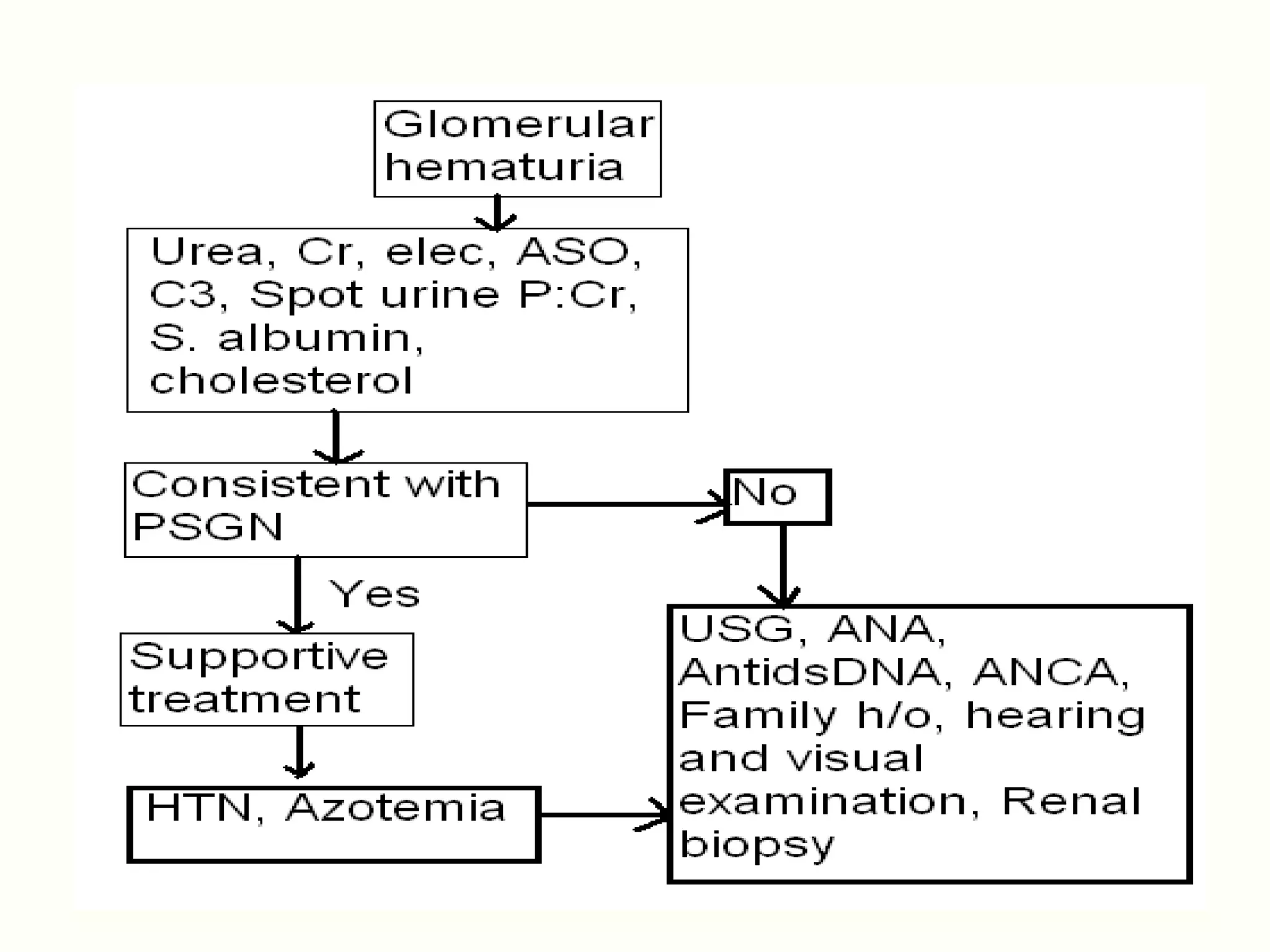
• CBC Step 1
• Electrolytes,Ca • Urine culture
• BUN/Cr Step 2
• Serum protein/albumin • Urine Ca/Cr
• Cholesterol • Renal/ bladder USG
• C3/C4 Step 3
• ASO/Anti-DNase B • Urinalysis: siblings, parents
• ANA • Serum electrolytes, Cr, Ca
• Antineutrophil antibody • If crystalluria, urolitiasis or
nephrocalcinosis:
• Throat/ skin culture
24-hr urine for Ca, Cr, Uric acid, oxalate
• 24-hour urine total protein
creatinine clearance • If hydronephrosis/pyelocaliectasis:
cystogram, renal scan
28.
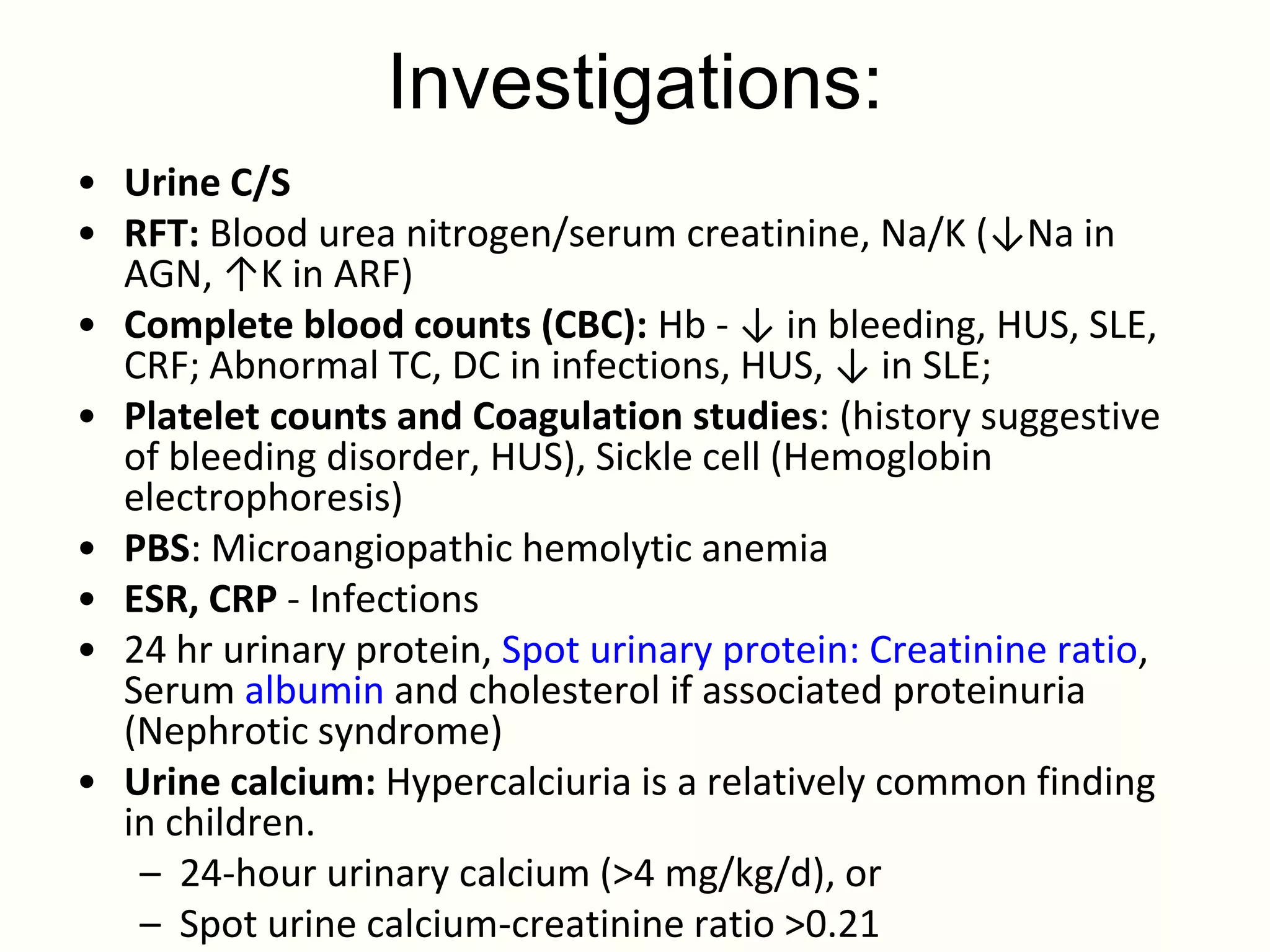
Investigations:
• Urine C/S
•RFT: Blood urea nitrogen/serum creatinine, Na/K (↓Na in
AGN, ↑K in ARF)
• Complete blood counts (CBC): Hb - ↓ in bleeding, HUS, SLE,
CRF; Abnormal TC, DC in infections, HUS, ↓ in SLE;
• Platelet counts and Coagulation studies: (history suggestive
of bleeding disorder, HUS), Sickle cell (Hemoglobin
electrophoresis)
• PBS: Microangiopathic hemolytic anemia
• ESR, CRP - Infections
• 24 hr urinary protein, Spot urinary protein: Creatinine ratio,
Serum albumin and cholesterol if associated proteinuria
(Nephrotic syndrome)
• Urine calcium: Hypercalciuria is a relatively common finding
in children.
– 24-hour urinary calcium (>4 mg/kg/d), or
– Spot urine calcium-creatinine ratio >0.21
29.
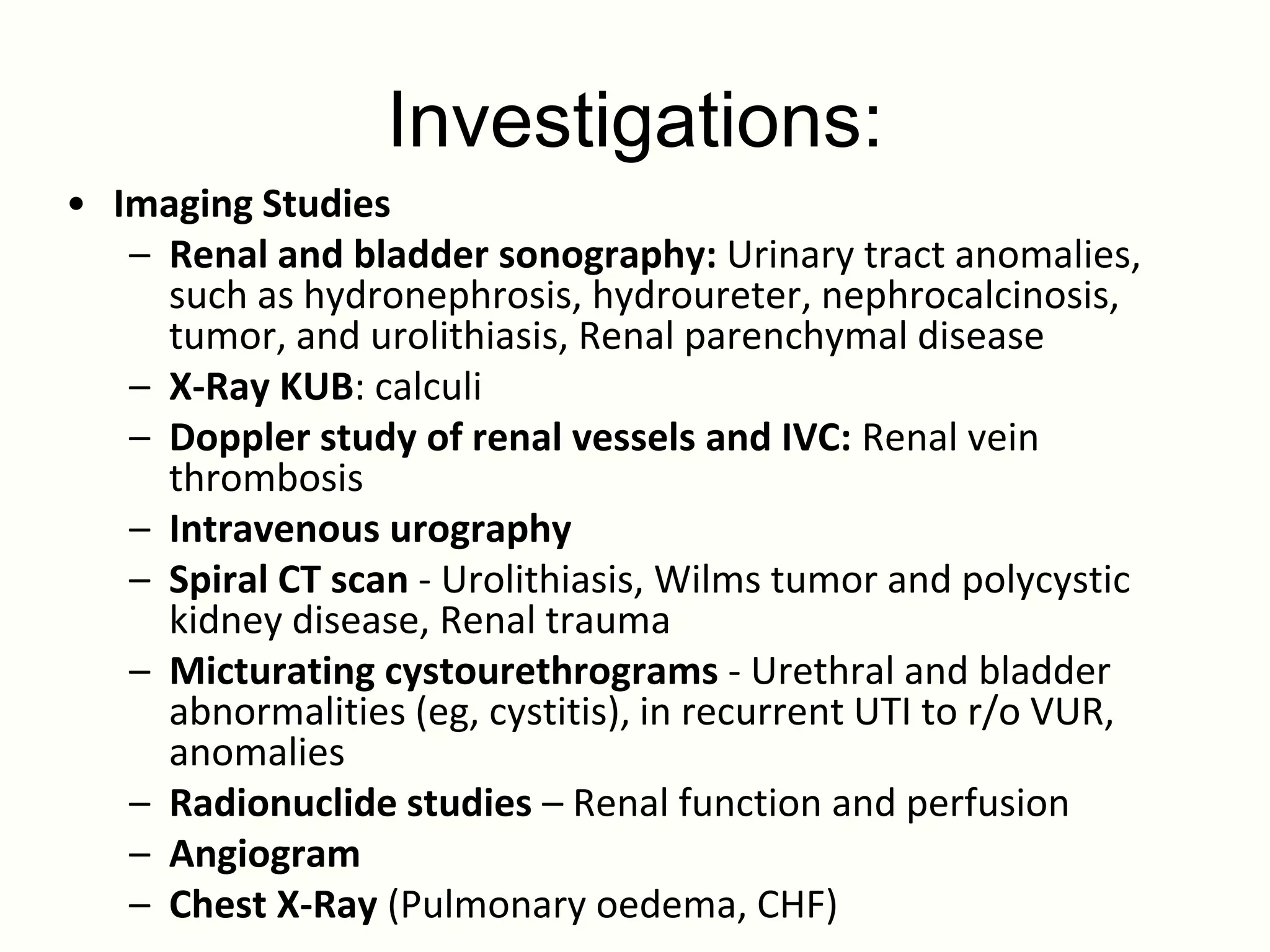
Investigations:
• Imaging Studies
– Renal and bladder sonography: Urinary tract anomalies,
such as hydronephrosis, hydroureter, nephrocalcinosis,
tumor, and urolithiasis, Renal parenchymal disease
– X-Ray KUB: calculi
– Doppler study of renal vessels and IVC: Renal vein
thrombosis
– Intravenous urography
– Spiral CT scan - Urolithiasis, Wilms tumor and polycystic
kidney disease, Renal trauma
– Micturating cystourethrograms - Urethral and bladder
abnormalities (eg, cystitis), in recurrent UTI to r/o VUR,
anomalies
– Radionuclide studies – Renal function and perfusion
– Angiogram
– Chest X-Ray (Pulmonary oedema, CHF)
30.
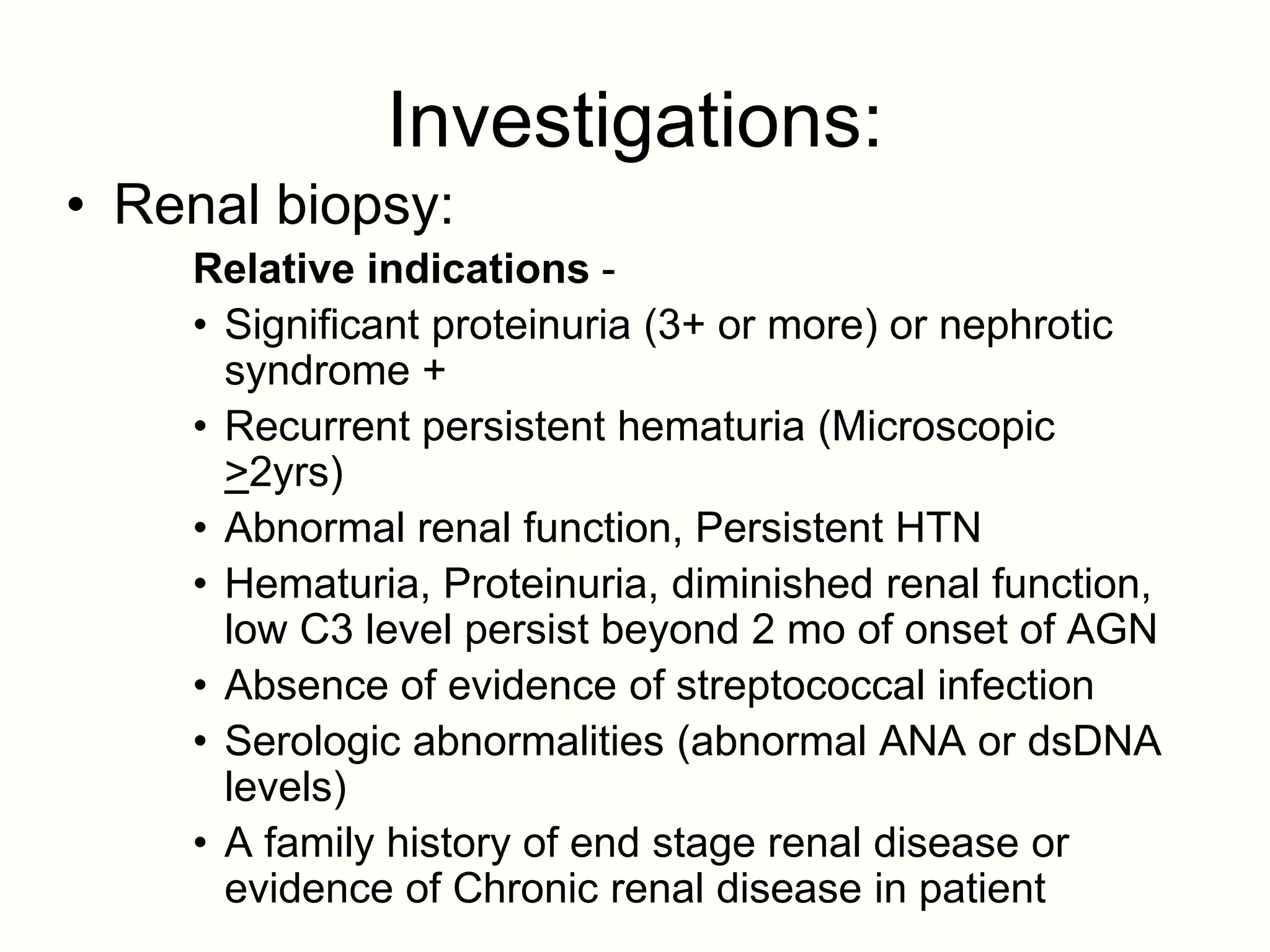
Investigations:
• Renal biopsy:
Relative indications -
• Significant proteinuria (3+ or more) or nephrotic
syndrome +
• Recurrent persistent hematuria (Microscopic
>2yrs)
• Abnormal renal function, Persistent HTN
• Hematuria, Proteinuria, diminished renal function,
low C3 level persist beyond 2 mo of onset of AGN
• Absence of evidence of streptococcal infection
• Serologic abnormalities (abnormal ANA or dsDNA
levels)
• A family history of end stage renal disease or
evidence of Chronic renal disease in patient
31.
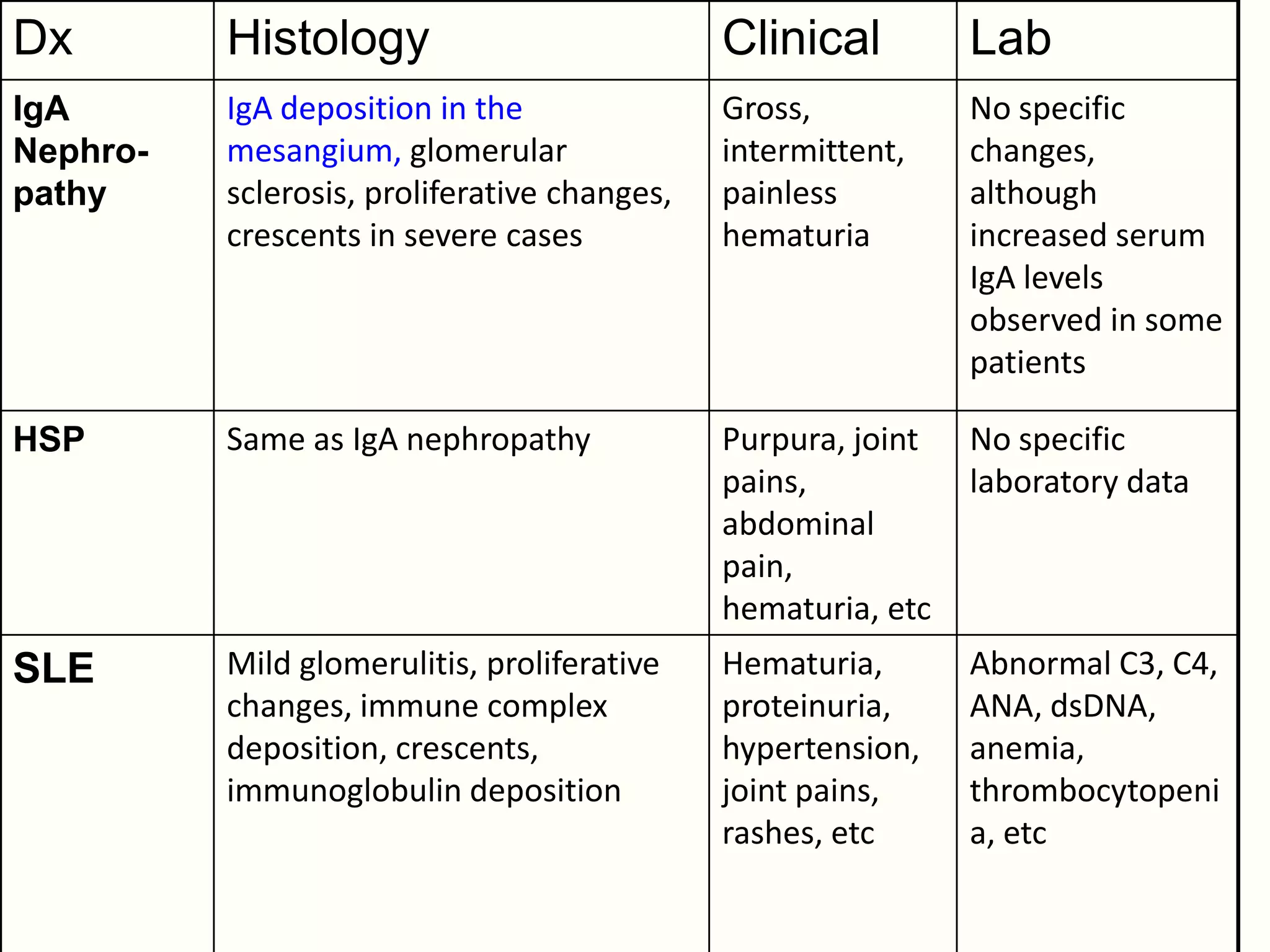
Dx Histology Clinical Lab
IgA IgA deposition in the Gross, No specific
Nephro- mesangium, glomerular intermittent, changes,
pathy sclerosis, proliferative changes, painless although
crescents in severe cases hematuria increased serum
IgA levels
observed in some
patients
HSP Same as IgA nephropathy Purpura, joint No specific
pains, laboratory data
abdominal
pain,
hematuria, etc
SLE Mild glomerulitis, proliferative Hematuria, Abnormal C3, C4,
changes, immune complex proteinuria, ANA, dsDNA,
deposition, crescents, hypertension, anemia,
immunoglobulin deposition joint pains, thrombocytopeni
rashes, etc a, etc
32.
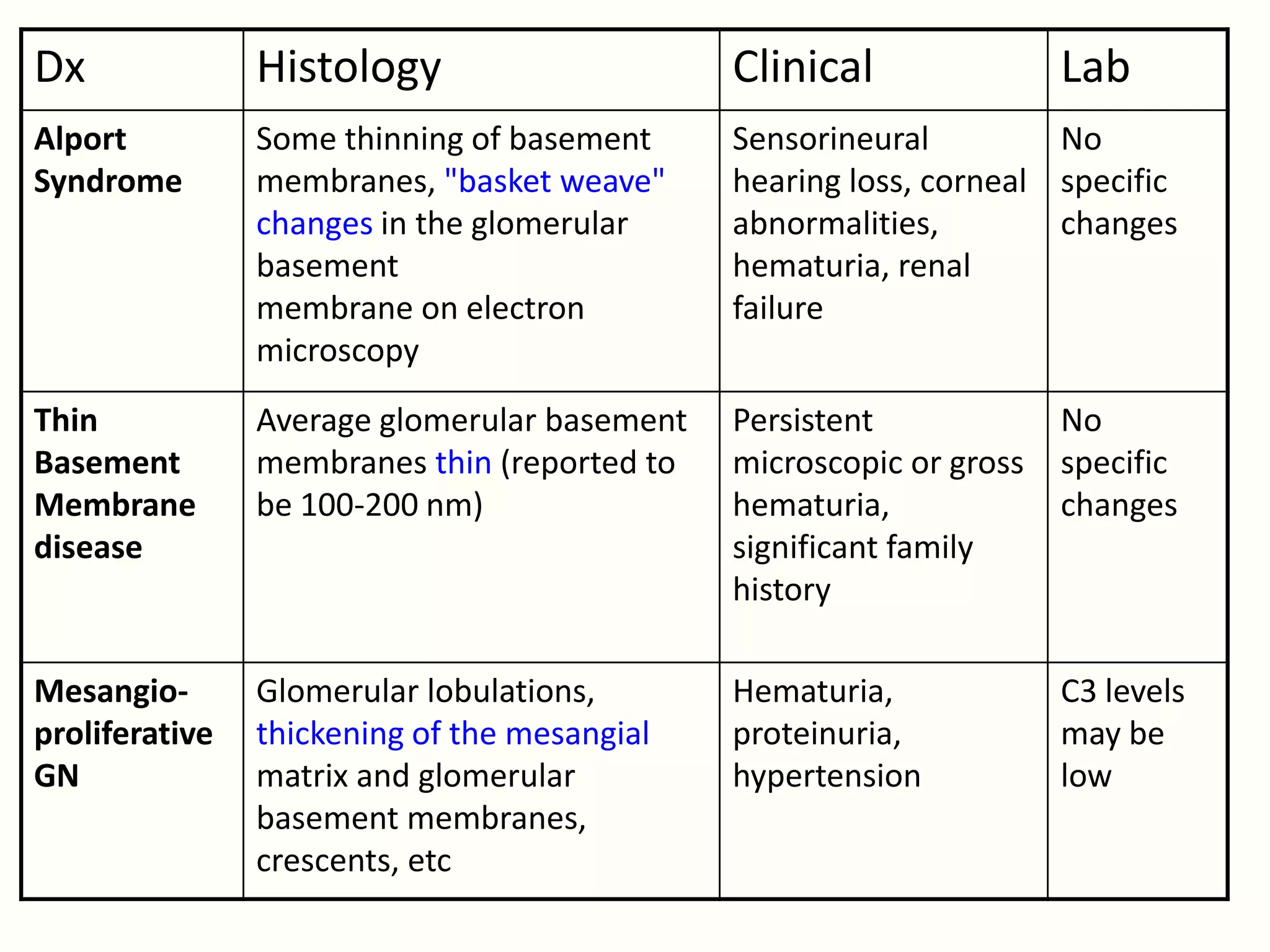
Dx Histology Clinical Lab
Alport Some thinning of basement Sensorineural No
Syndrome membranes, "basket weave" hearing loss, corneal specific
changes in the glomerular abnormalities, changes
basement hematuria, renal
membrane on electron failure
microscopy
Thin Average glomerular basement Persistent No
Basement membranes thin (reported to microscopic or gross specific
Membrane be 100-200 nm) hematuria, changes
disease significant family
history
Mesangio- Glomerular lobulations, Hematuria, C3 levels
proliferative thickening of the mesangial proteinuria, may be
GN matrix and glomerular hypertension low
basement membranes,
crescents, etc
33.
Investigations:
• Cystourethroscopy: Terminalhematuria,
disturbances of micturition, suprapubic pain
(Only if strong suspicion of bladder ulceration,
tumours)
• Screening of first degree relatives in persistent
hematuria
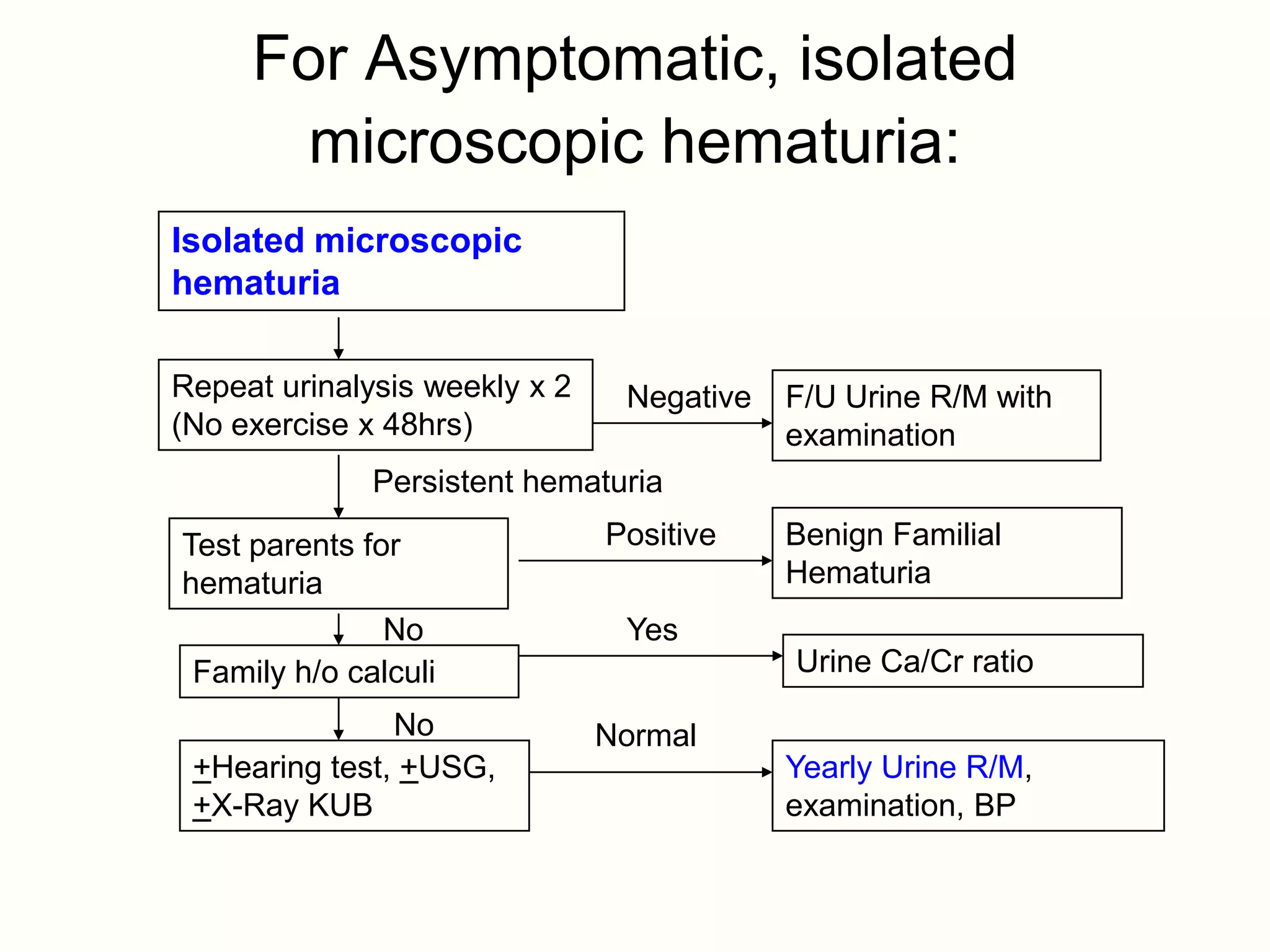
For Asymptomatic, isolated
microscopic hematuria:
Isolated microscopic
hematuria
Repeat urinalysis weekly x 2 Negative F/U Urine R/M with
(No exercise x 48hrs) examination
Persistent hematuria
Test parents for Positive Benign Familial
hematuria Hematuria
No Yes
Family h/o calculi Urine Ca/Cr ratio
No Normal
+Hearing test, +USG, Yearly Urine R/M,
+X-Ray KUB examination, BP
39.
Management:
• According tocause:
– Reassurance and F/U
– Treat cystitis, pyelonephritis, AGN: Antibiotics
– Supportive treatment: Diuretics, Fluid and salt
restriction, Antihypertensives
– Monitoring – BP, I/O, weight, Urine R/M
– Treat Hyperkalemia, ARF, CHF, acidosis, fluid
overload, HTN and its complications
– ACE inhibitors useful in proteinuria
– Immunosuppressive therapy: Depending on cause
(Steroids, cyclophosphamide)
40.
Management:
– Idiopathic Hypercalciuria:Hydrochlorothiazide, Potassium
citrate, Sodium restriction
– Calculi: Plenty of water
– ESRD: Dialysis, Renal transplantation
– Correct thrombocytopenia, anemia, coagulation factor
deficiency
– Renal vein thrombosis: Anticoagulant therapy or
thrombectomy may be needed
– Surgical correction: Calculi, PUJ obstruction, Posterior
urethral valves, Wilms tumour
41.
References:
• Nelson Textbookof Pediatrics, 19th Ed
• Nelson Essentials of Pediatrics, 6th Ed
• O.P. Ghai Essential pediatrics, 7th Ed
• Pediatric Nephrology, Shrivastava, Bagga,
4th Ed
• Japanese Society of Nephrology 2007
• Indian J Pediatrics 1999; 66 : 207-214
• Various Websites