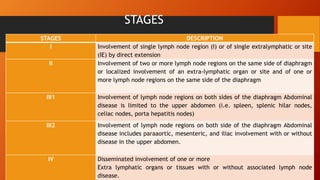
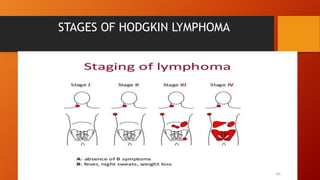
This document discusses Hodgkin lymphoma and non-Hodgkin lymphoma. It covers the causes, signs and symptoms, stages of disease, diagnosis, and treatment for both types of lymphoma. Hodgkin lymphoma is characterized by Reed-Sternberg cells and can be nodular lymphocytic or classical. Non-Hodgkin lymphoma involves either B cells or T cells and includes subtypes like diffuse large B-cell lymphoma and Burkitt lymphoma. Staging evaluates extent of disease spread. Diagnosis involves biopsies and imaging tests. Treatment primarily consists of chemotherapy for children, while chemotherapy and radiation are used in adults.