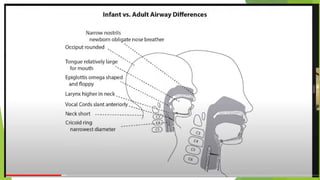
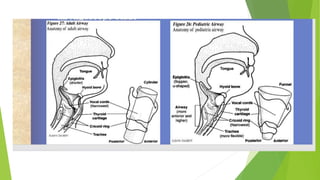
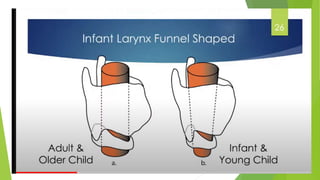
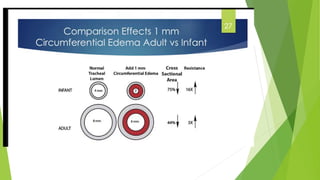
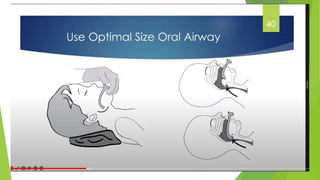
The document discusses pediatric airway management, highlighting significant anatomical and physiological differences between children and adults that impact anesthesia techniques. Key factors include the larger relative size of the child's head and tongue, obligate nasal breathing in infancy, and the unique shape of the larynx and epiglottis. Recommendations for airway assessment and management are provided, stressing the importance of tailored approaches for pediatric patients to ensure safety during procedures.