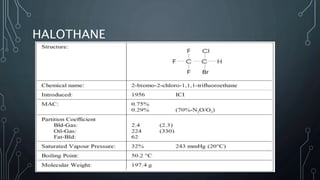
The document provides a history of anesthetic agents, beginning with diethyl ether in 1846 and progressing to modern volatile agents like sevoflurane. It discusses the properties of each agent that made them viable or led to their discontinuation. It also defines the minimum alveolar concentration (MAC) concept for measuring anesthetic potency based on immobilization during incision. Factors that increase or decrease MAC values are outlined.