ANATOMY
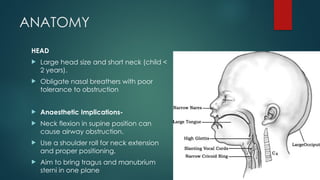
HEAD
Large headsize and short neck (child <
2 years).
Obligate nasal breathers with poor
tolerance to obstruction
Anaesthetic Implications-
Neck flexion in supine position can
cause airway obstruction.
Use a shoulder roll for neck extension
and proper positioning.
Aim to bring tragus and manubrium
sterni in one plane
3.
Tongue
Small mouth,large tongue
Difficult to visualize larynx
Anaesthetic Implications-
Likelihood of upper airway obstruction
Use an oro/nasopharyngeal airway to
maintain airway patency
4.
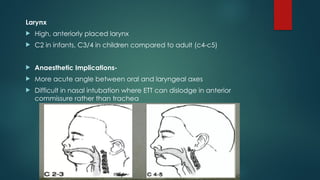
Larynx
High, anteriorlyplaced larynx
C2 in infants, C3/4 in children compared to adult (c4-c5)
Anaesthetic Implications-
More acute angle between oral and laryngeal axes
Difficult in nasal intubation where ETT can dislodge in anterior
commissure rather than trachea
5.
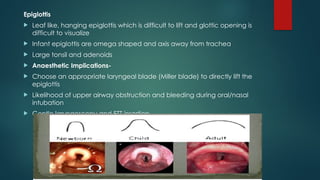
Epiglottis
Leaf like,hanging epiglottis which is difficult to lift and glottic opening is
difficult to visualize
Infant epiglottis are omega shaped and axis away from trachea
Large tonsil and adenoids
Anaesthetic Implications-
Choose an appropriate laryngeal blade (Miller blade) to directly lift the
epiglottis
Likelihood of upper airway obstruction and bleeding during oral/nasal
intubation
Gentle laryngoscopy and ETT insertion
6.
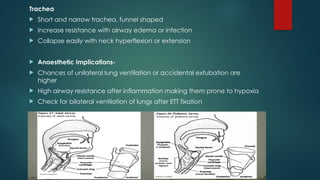
Trachea
Short andnarrow trachea, funnel shaped
Increase resistance with airway edema or infection
Collapse easily with neck hyperflexion or extension
Anaesthetic Implications-
Chances of unilateral lung ventilation or accidental extubation are
higher
High airway resistance after inflammation making them prone to hypoxia
Check for bilateral ventilation of lungs after ETT fixation
7.
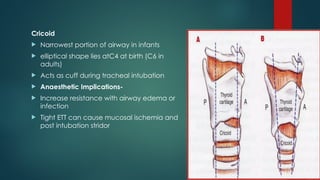
Cricoid
Narrowest portionof airway in infants
elliptical shape lies atC4 at birth (C6 in
adults)
Acts as cuff during tracheal intubation
Anaesthetic Implications-
Increase resistance with airway edema or
infection
Tight ETT can cause mucosal ischemia and
post intubation stridor
8.
Neck
Short thickneck makes localization of cricothyroid membrane
difficult
Anaesthetic Implications-
Cricothyroidotomy difficult in children aged < 8 years.
Higher risk of puncture of posterior tracheal wall
Pre-define and mark the landmarks if a difficult airway is
anticipated.
Surgical tracheotomy preferred over scalpel technique in a ‘can’t
intubate can’t ventilate’ (CICV) scenario in children aged <8 years
9.
Chest wall
Horizontalribs
More A-P diameter
Increase compliance due to weak rib cage
Diaphragmatic breathing
Anaesthetic Implications-
FRC determined solely by elastic recoil of lungs
Chest wall collapse with negative pressure
10.
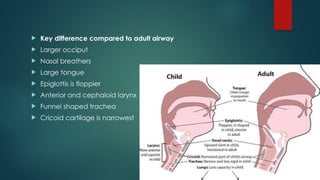
Key differencecompared to adult airway
Larger occiput
Nasal breathers
Large tongue
Epiglottis is floppier
Anterior and cephaloid larynx
Funnel shaped trachea
Cricoid cartilage is narrowest
11.
PHYSIOLOGY
High metabolicrate (5-8 ml/kg/min)
Oxygen consumption of infant (6ml/kg/min) is twice that of adult
(3ml/kg/min).
Tidal volume is relatively fixed (6-7ml/kg/min)
Minute ventilation is more dependent on raspiratory rate than tidal
volume
Lung compliance is less while chest compliance is more than adult.
Lack of type 1 muscle fibers
Higher vagal tone
Rib cage is more horizontal
12.
Anaesthetic Implications-
Higher O2 consumption and less apnoea time to desaturation
After induction of anaesthesia, loss of FRC causes atelectasis and
rapid desaturation
Prone to early fatigue adding to early desaturation
Restricted deep breathing
More chances of bradycardia during airway instrumentation.
Bradycardia leading to low cardiac output further aggravating
hypoxemia
Hypoxia itself causes bradycardia
13.
Airway assessment
Lookfrom afar-
Is the chest moving ?
Can you hear the breath sounds ?
Are there any abnormal airway sounds (stridor, snoring) ?
Is there increased respiratory effort with no airway or breath
sounds ?
14.
Medical History
URTI– laryngospasm , bronchospasm, desaturation during
anaesthesia
Snoring – adenoid hypertrophy, OSA, upper airway obstruction
Chronic cough – subglottic stenosis, tracheoesophageal fistula.
Productive cough – pneumonia, bronchitis.
Sudden onset of new cough – foreign body aspiration.
Inspiratory stridor – macroglossia, laryngeal web,
laryngomalacia, extra thoracic foreign body.
Hoarse voice – laryngitis, vocal cord palsy, papillomatosis
Asthma – bronchospasm
15.
Medical History
Repeatedpneumonia – GERD, bronchiectasis, tracheoesophageal
fistula, congenital heart disease
Atopy , allergy – increase airway reactivity
Congenital syndromes – Pierre Robin syndrome, Treacher Collins,
Klippel Feil, Down syndrome etc.
Previous anaesthetic problem
Environmental smokers
16.
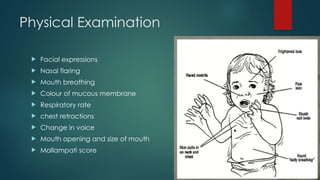
Physical Examination
Facialexpressions
Nasal flaring
Mouth breathing
Colour of mucous membrane
Respiratory rate
chest retractions
Change in voice
Mouth opening and size of mouth
Mallampati score
17.
Physical Examination
Looseor missing teeth
Size and configuration of mandible and palate
Inspiratory and expiratory stridor (foreign body , vascular ring )
Prolonged expiration ( lower airway disease)
Baseline oxygen saturation
18.
Airway Management
Airwaypatency improved on –
Suction nose and oropharynx
Reposition child
Head tilt, chin lift ,jaw thrust
Use airway adjunct (NPA, OPA)
Bag and mask ventilation
Intubation
19.
Requirement for airwaycart for a
child (SOAPME)
Suction -Working, effective suction and appropriate size suction catheter.
Oxygen -Oxygen source, tubing, flow meters.
Airway Devices -Appropriate sizes of face masks, self-inflating bag,
oropharyngeal and nasopharyngeal airways, laryngoscope blades
(MacIntosh: 1, Miller: 0,1,2) video laryngoscope, supraglottic airway (SGA,
1st and 2nd generation), ETT, intubating stylet, tube exchanger, FOB.
Positioning -“Sniffing” position, shoulder roll for smaller children.
Pharmacy -IV anaesthetics, muscle relaxants. Resuscitation drugs:
adrenaline, flumazenil.
Monitors -SpO2, ECG, NIBP, EtCO2, RR, temperature.
Equipment -Defibrillator, cricothyroidotomy, tracheostomy sets for
emergency front of neck access (FONA)
21.
SUCTIONING
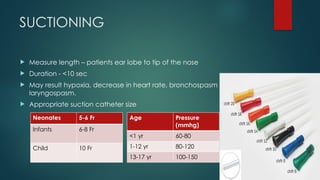
Measure length– patients ear lobe to tip of the nose
Duration - <10 sec
May result hypoxia, decrease in heart rate, bronchospasm ,
laryngospasm.
Appropriate suction catheter size
Neonates 5-6 Fr
Infants 6-8 Fr
Child 10 Fr
Age Pressure
(mmhg)
<1 yr 60-80
1-12 yr 80-120
13-17 yr 100-150
22.
Artificial airway
Oralairway
Nasal airway
Appropriate size is the key
Too small – will not adequately displace the tongue
Too large – may obstruct larynx or interfere with mask fit
23.
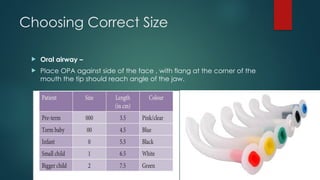
Choosing Correct Size
Oral airway –
Place OPA against side of the face , with flang at the corner of the
mouth the tip should reach angle of the jaw.
24.
Choosing Correct Size
Nasal airway-
Distance from nares to angle of mandible approximates
the proper length
NPA sizes from 12fr to 36Fr.
Shortened endotracheal tube is used
Avoid in case of adenoid hypertrophy –bleeding and
trauma
25.
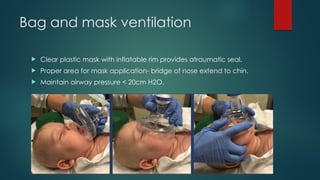
Bag and maskventilation
Clear plastic mask with inflatable rim provides atraumatic seal.
Proper area for mask application- bridge of nose extend to chin.
Maintain airway pressure < 20cm H2O.
26.
Bag and maskventilation
Place fingers on mandible to avoid
compressing pharyngeal space.
Had on ventilation bag at all times
to monitor effectiveness of
spontaneous breaths.
Continuous positive pressure when
needed to maintain airway
patency.
27.
Bagging unit
Neonate– 250- 500 ml
Infant – 500ml
Paediatric bag – 500-1000ml
Small adult – 1L
Adult bag – 1.5 – 2 L
28.
Patient Position
Aneutral “sniffing” position without
hyperextension is appropriate for infants
and toddlers.
Avoid extreme hyperextension in infants as
it may cause airway obstruction
In patients with head or neck injuries,
maintain the neck in a neutral position.
29.
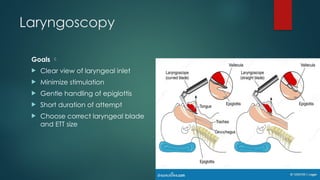
Laryngoscopy
Goals
Clearview of laryngeal inlet
Minimize stimulation
Gentle handling of epiglottis
Short duration of attempt
Choose correct laryngeal blade
and ETT size
30.
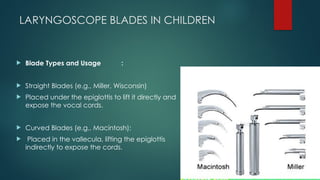
LARYNGOSCOPE BLADES INCHILDREN
Blade Types and Usage :
Straight Blades (e.g., Miller, Wisconsin)
Placed under the epiglottis to lift it directly and
expose the vocal cords.
Curved Blades (e.g., Macintosh):
Placed in the vallecula, lifting the epiglottis
indirectly to expose the cords.
31.
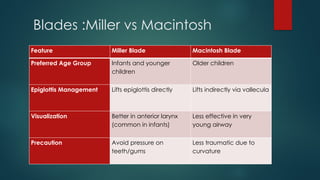
Blades :Miller vsMacintosh
Feature Miller Blade Macintosh Blade
Preferred Age Group Infants and younger
children
Older children
Epiglottis Management Lifts epiglottis directly Lifts indirectly via vallecula
Visualization Better in anterior larynx
(common in infants)
Less effective in very
young airway
Precaution Avoid pressure on
teeth/gums
Less traumatic due to
curvature
32.
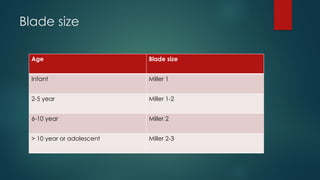
Blade size
Age Bladesize
Infant Miller 1
2-5 year Miller 1-2
6-10 year Miller 2
> 10 year or adolescent Miller 2-3
33.
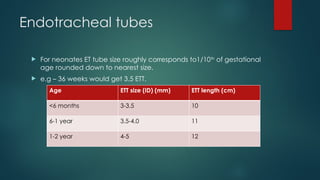
Endotracheal tubes
Forneonates ET tube size roughly corresponds to1/10th
of gestational
age rounded down to nearest size.
e.g – 36 weeks would get 3.5 ETT.
Age ETT size (ID) (mm) ETT length (cm)
<6 months 3-3.5 10
6-1 year 3.5-4.0 11
1-2 year 4-5 12
34.
2-12 years–
Size :
Uncuffed ET tube : (age in years / 4)+4
Cuffed ET tube : ( age in years / 4) + 3.5
Length :
(age in years / 2) + 12
35.
Cuffed V/S Uncuffedtube
Uncuffed ETT Recommended: In children < 8
years to avoid:
Post-extubation stridor
Subglottic stenosis
Cuffed ETT Preferable When:
High risk of aspiration(e.g., bowel
obstruction)
Low lung compliance(e.g., ARDS,
pneumoperitoneum, CO insufflation of
₂
thorax, CABG)
Need precise control of ventilation &
pCO (e.g., ↑ intracranial pressure, single
₂
ventricle physiology)
36.
Cuffed V/S Uncuffedtube
Disadvantages of Cuffed ETT:
Smaller size = ↑ airway resistance
↑ Work of breathing
Poorly paediatric design
Need to keep Cuff pressure must be < 25 cm H O
₂
Disadvantages of Uncuffed ETT:
Frequent tube changes in long-term use
Aesthetic gas leak into environment
Needs higher fresh gas flow (> 2 L/min)
↑ Aspiration risk
Acute deterioration postintubation
Displaced ETT : ETT may be in trachea or in right or left main
bronchus.
Obstruction of ETT : secretions, blood, pus, foreign body, kinked ETT.
Pneumothorax : simple , tension.
Equipment failure : disconnection of O2 source, leaks in vent circuits,
loss of power or vent malfunction.
39.
PREDICTORS OF DIFFICULTAIRWAY
LEMON
Look : short neck , large tongue, micrognathia
Evaluate : 3-3-2
3 fingers breadth of mouth opening
3 fingers breadth submental to hyoid
2 fingers breadth hyoid to thyroid
Mallampati score
Obstruction
Neck mobility
40.
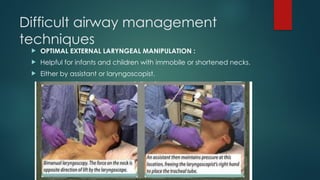
Difficult airway management
techniques
OPTIMAL EXTERNAL LARYNGEAL MANIPULATION :
Helpful for infants and children with immobile or shortened necks.
Either by assistant or laryngoscopist.
41.
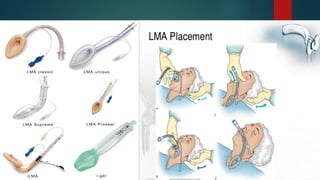
Laryngeal Mask
Supraglotticairway device developed by Dr Archie Brain
Useful in difficult airway situations.
Easy to place
Used in any age
Contraindication : Gag reflex
Foreign body
Airway obstruction
High ventilation pressure
Disadvantage : laryngospasm, aspiration.
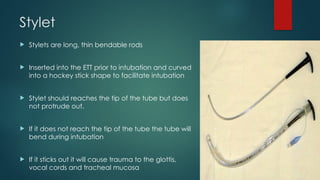
Stylet
Stylets arelong, thin bendable rods
Inserted into the ETT prior to intubation and curved
into a hockey stick shape to facilitate intubation
Stylet should reaches the tip of the tube but does
not protrude out.
If it does not reach the tip of the tube the tube will
bend during intubation
If it sticks out it will cause trauma to the glottis,
vocal cords and tracheal mucosa
45.
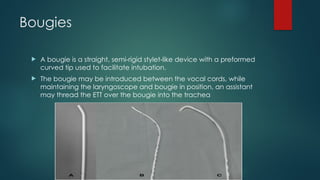
Bougies
A bougieis a straight, semi-rigid stylet-like device with a preformed
curved tip used to facilitate intubation.
The bougie may be introduced between the vocal cords, while
maintaining the laryngoscope and bougie in position, an assistant
may thread the ETT over the bougie into the trachea
46.
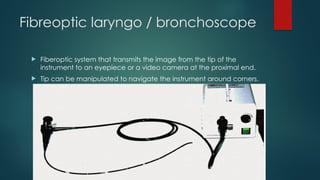
Fibreoptic laryngo /bronchoscope
Fiberoptic system that transmits the image from the tip of the
instrument to an eyepiece or a video camera at the proximal end.
Tip can be manipulated to navigate the instrument around corners.
47.
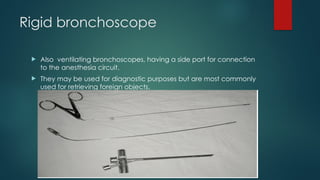
Rigid bronchoscope
Alsoventilating bronchoscopes, having a side port for connection
to the anesthesia circuit.
They may be used for diagnostic purposes but are most commonly
used for retrieving foreign objects.
48.
Video laryngoscope
Themost commonly
available video
laryngoscopes for use in
children are:
Airtraq optical
laryngoscope,
Glidescope (Verathan
Medical), CMac (Karl
Storz), Truview (Truphatek)
and Pentax AWS (Pentax).
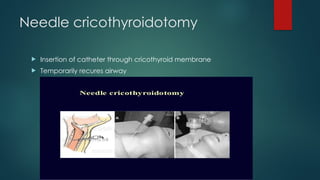
Cricothyroidotomy
<5 yearsof age :
Needle cricothyroidotomy and bag ventilation
5-10 years of age :
Needle cricothyroidotomy and bag ventilation
If oxygen saturation inadequate, transtracheal jet ventilation
>10 years of age :
Needle cricothyroidotomy with TTJV
Surgical cricothyroidotomy – contraindicated <10 years of age