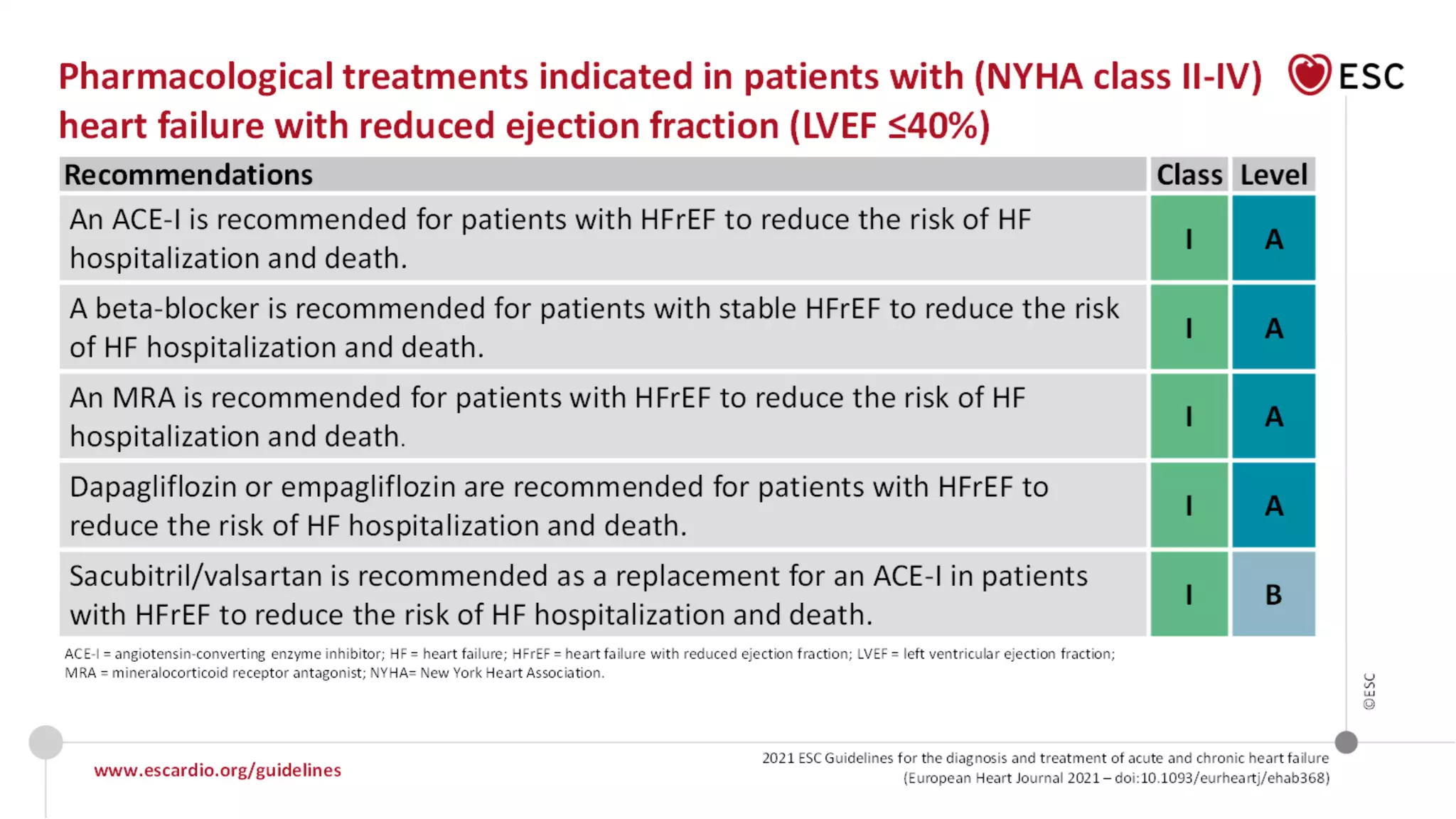
The document discusses a case study of a patient with heart failure with reduced ejection fraction (HFREF) and outlines the efficacy of sacubitril/valsartan compared to enalapril in treating heart failure, as demonstrated in the PARADIGM-HF trial. The trial showed significant improvements in mortality and hospitalization rates for patients treated with sacubitril/valsartan, highlighting its benefits over traditional therapies. It emphasizes the importance of adhering to updated therapeutic guidelines and showcases various clinical outcomes related to heart failure treatments.