Download as PDF, PPTX

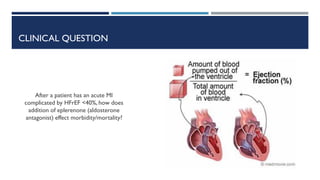
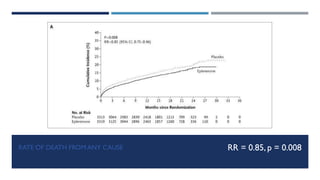
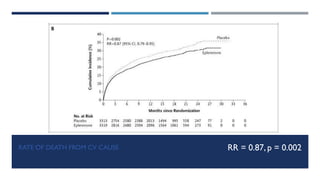
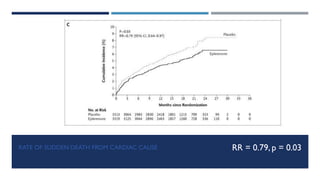
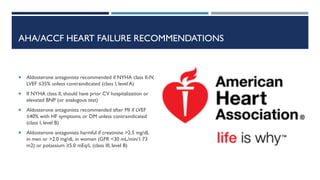


- The EPHESUS trial randomized over 6,000 patients who had a myocardial infarction with reduced left ventricular ejection fraction (<40%) within 3-14 days to eplerenone or placebo in addition to standard therapy. - At 16 months follow up, eplerenone reduced the risk of death from any cause by 15% and death from cardiovascular causes by 13% compared to placebo. - Eplerenone was generally well tolerated but increased the risk of hyperkalemia compared to placebo.










![Heart failure – an update [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/heartfailureanupdateautosaved-110321012825-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
















































































