

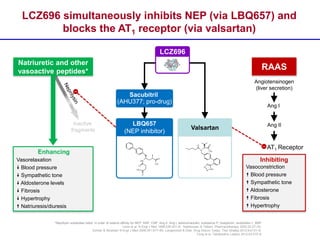
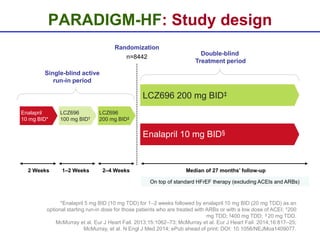
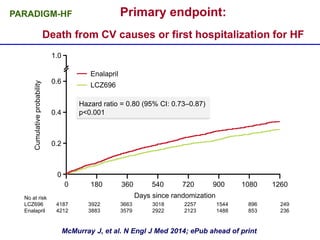
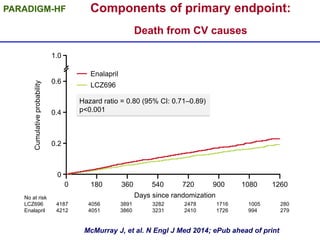
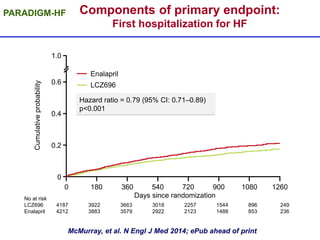
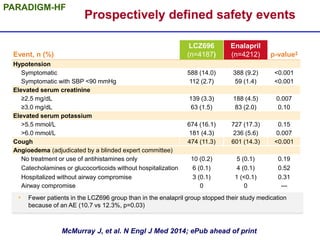
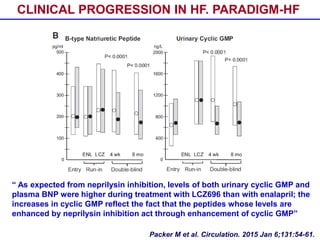
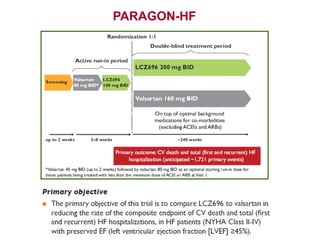
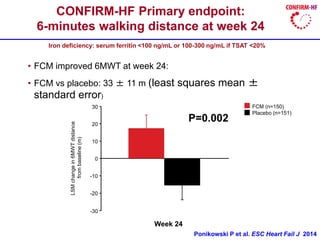
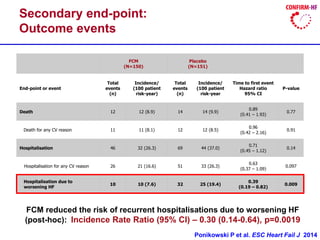
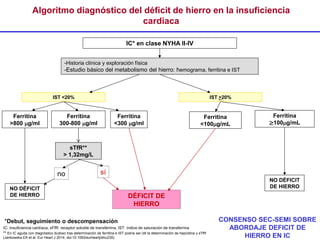
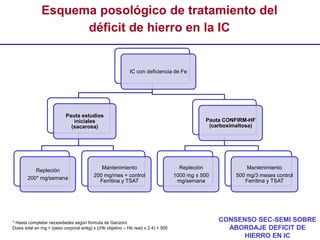
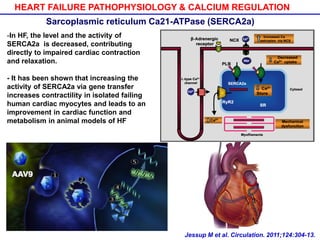
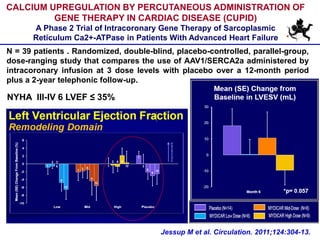
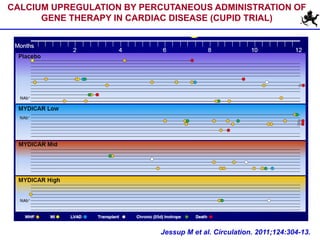
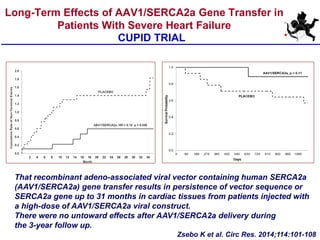
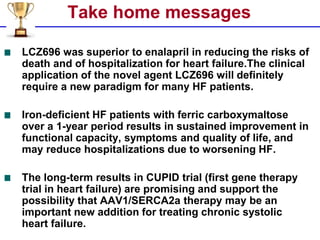

Dr. Nicolás Manito discusses innovative strategies in heart failure management, emphasizing the superiority of lcz696 over enalapril in reducing cardiovascular mortality and hospitalization rates. The use of ferric carboxymaltose in iron-deficient heart failure patients has shown substantial improvements in functional capacity, while gene therapy trials like CUPID suggest promising long-term effects for treating chronic systolic heart failure. The document highlights the need for a paradigm shift in the treatment approach for heart failure patients, integrating new therapeutic options.