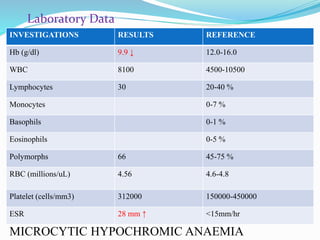
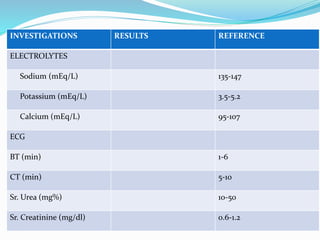
This case presentation discusses a 1 year and 2 month old female child admitted to the hospital with febrile seizures. The child presented with a history of fever and two episodes of abnormal movements involving stiffening and up rolling of the eyes. On examination, the child was conscious with tachycardia and normal temperature. Laboratory investigations revealed microcytic hypochromic anemia. The child was diagnosed with febrile seizures and treated with intravenous antibiotics, anticonvulsants and antipyretics. The child improved with treatment and was discharged on oral medications including anticonvulsants and antipyretics to prevent recurrence of seizures during fever.













































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)



