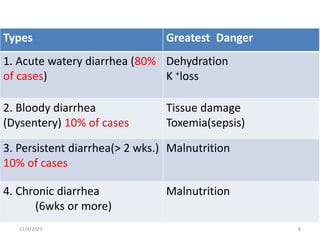
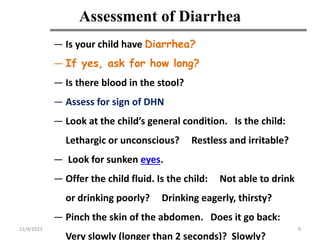
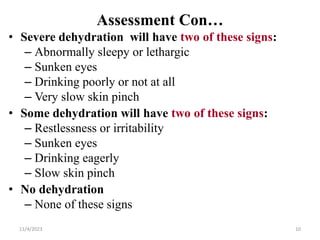
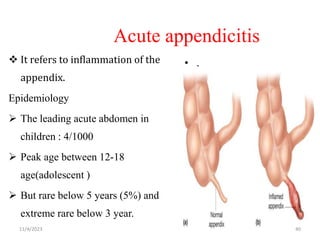
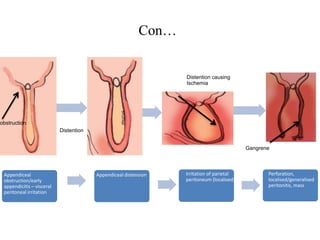
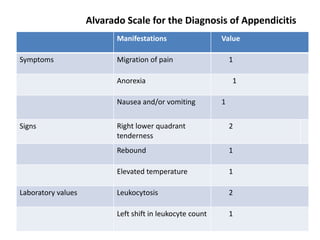
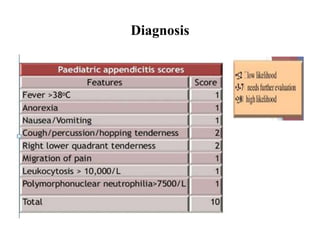
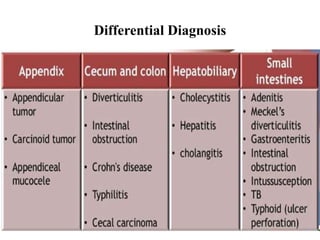
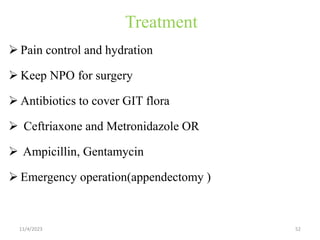
The document discusses common childhood gastrointestinal problems such as gastroenteritis, diarrhea, intestinal obstruction, and appendicitis. It provides details on the causes, symptoms, diagnosis, and treatment of each condition. For diarrhea specifically, it describes the various types, causes, assessment techniques involving dehydration status, and treatment approaches including oral rehydration and continued feeding. Intestinal obstruction is classified and common causes in children like intussusception are explained. For appendicitis, it notes the signs, diagnostic tests, and surgical treatment required.