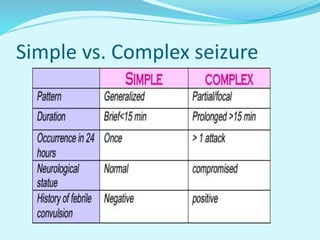
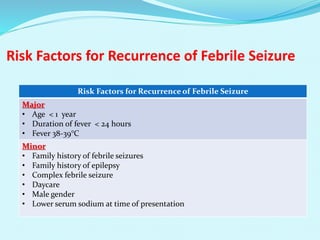
Febrile seizures are the most common seizure disorder in children, occurring in those aged 6 months to 5 years, characterized by a fever without central nervous system infection. The document discusses types of febrile seizures, their risk factors, and evaluation methods, including when to perform lumbar puncture and EEG. It also addresses treatment options, emphasizing that antiepileptic therapy is generally not recommended, and advising on how to manage febrile seizures at home.













































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)












