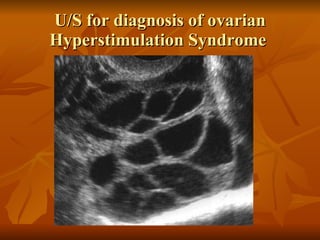
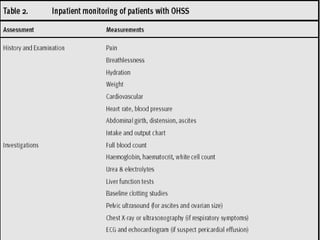
Ovarian Hyperstimulation Syndrome (OHSS) is a condition characterized by ovarian enlargement and fluid accumulation in the abdomen and chest. It occurs most commonly as a complication of ovulation induction treatments. The document discusses risk factors, pathogenesis, classification, complications, prevention, and treatment of OHSS. Prevention focuses on predicting risk through endocrine and ultrasound monitoring to determine the optimal time for ovulation trigger and modifying stimulation protocols if needed. Treatment involves fluid management, symptom relief, and in severe cases hospitalization and close monitoring.







![Thank you E.MAIL :: [email_address]](https://image.slidesharecdn.com/ovarianhyperstimulationsyndrome-1218074147410352-9/85/Ovarian-Hyperstimulation-Syndrome-43-320.jpg)
































































































