Downloaded 193 times


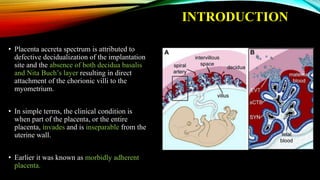
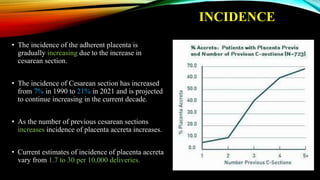
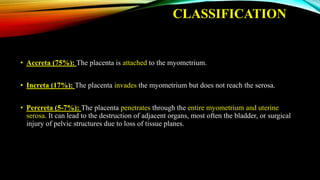
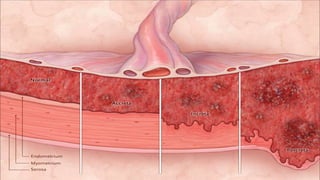






1) Placenta accreta spectrum disorders occur when the placenta invades and is inseparable from the uterine wall, posing risks of heavy bleeding. The incidence has increased 10-fold in recent decades due to rising c-sections. 2) Risk factors include placenta previa, prior c-sections, and other uterine surgeries. Early diagnosis using ultrasound and MRI is important for management planning. 3) Management involves a multidisciplinary approach, with the goal of minimizing blood loss through techniques like arterial embolization and hysterectomy if needed. Conservative management is sometimes attempted but carries risks if failed.
















































































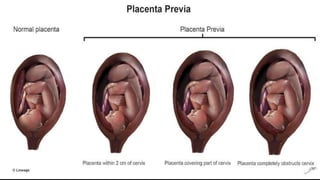
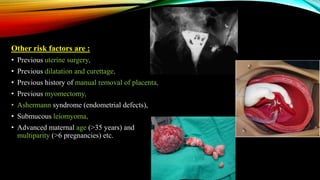
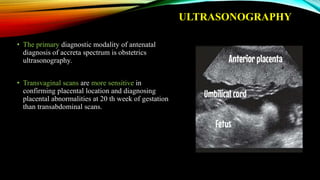
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

