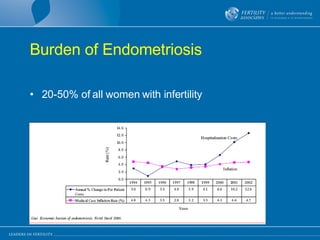
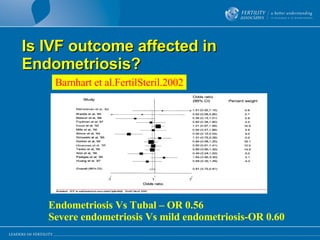
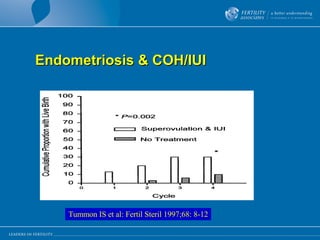
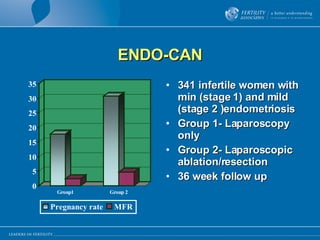
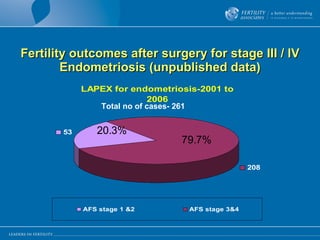
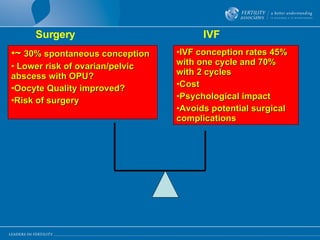
This document discusses whether surgery improves fertility outcomes for women with endometriosis. It reviews several studies that have looked at IVF success rates and spontaneous pregnancy rates after surgery for mild versus severe endometriosis. The document also presents unpublished data from a study of 261 women who underwent laparoscopic excision for stage III/IV endometriosis, finding a 79.7% spontaneous pregnancy rate. It concludes that while surgery is generally recommended for stage I/II endometriosis, the role of surgery for stage III/IV endometriosis remains controversial in improving fertility outcomes due to a lack of large, prospective studies.


































































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





