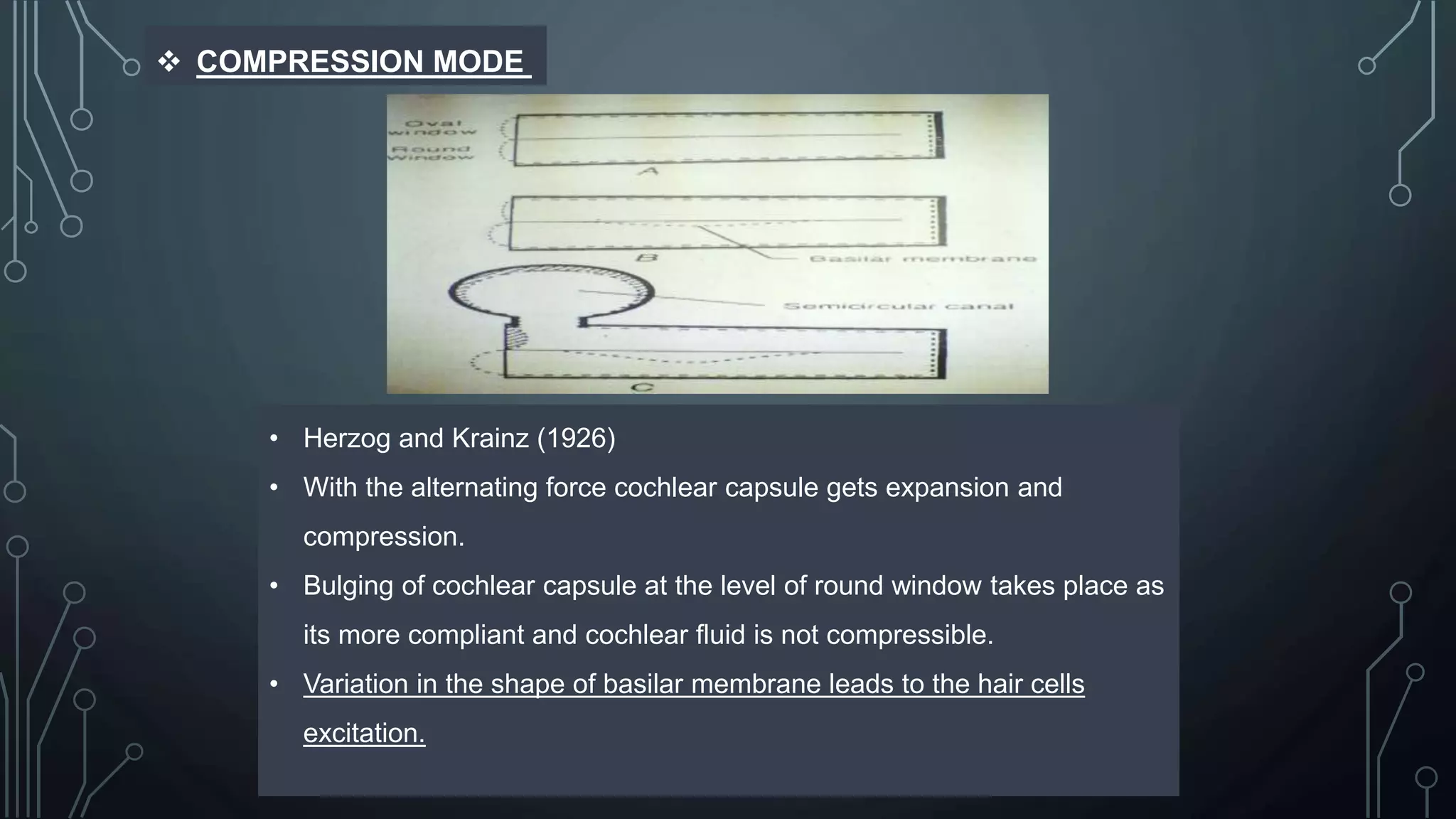
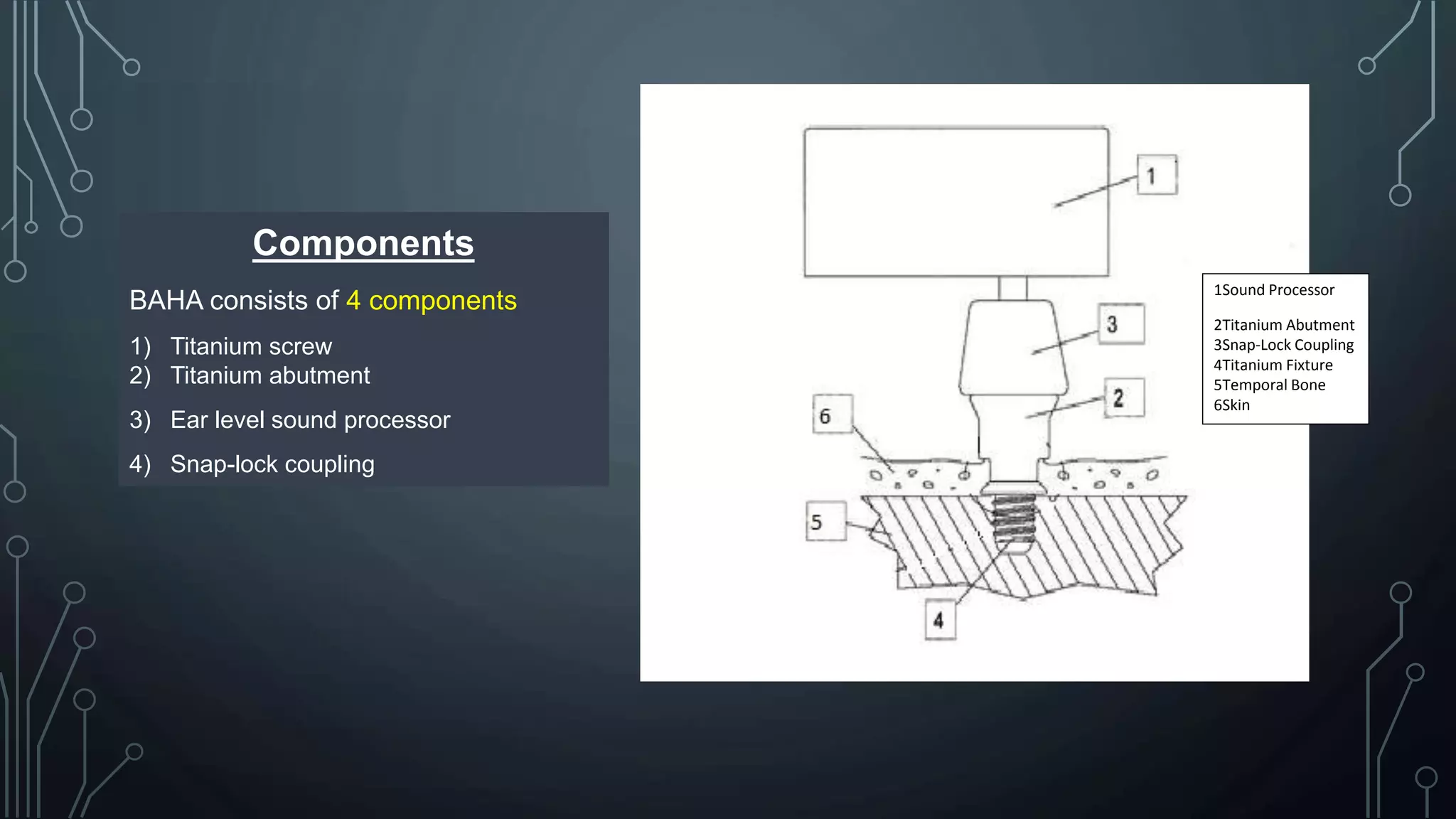
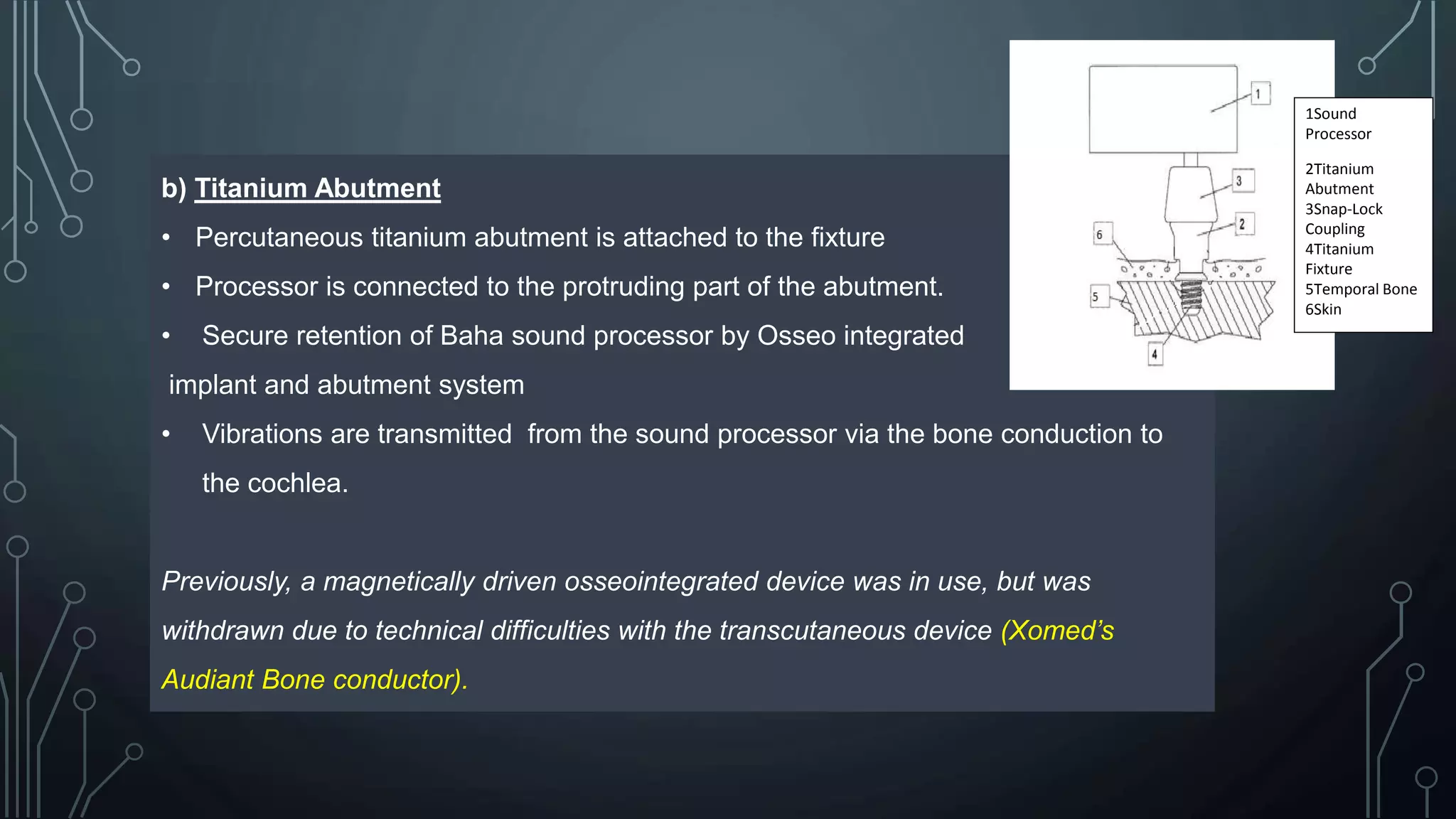
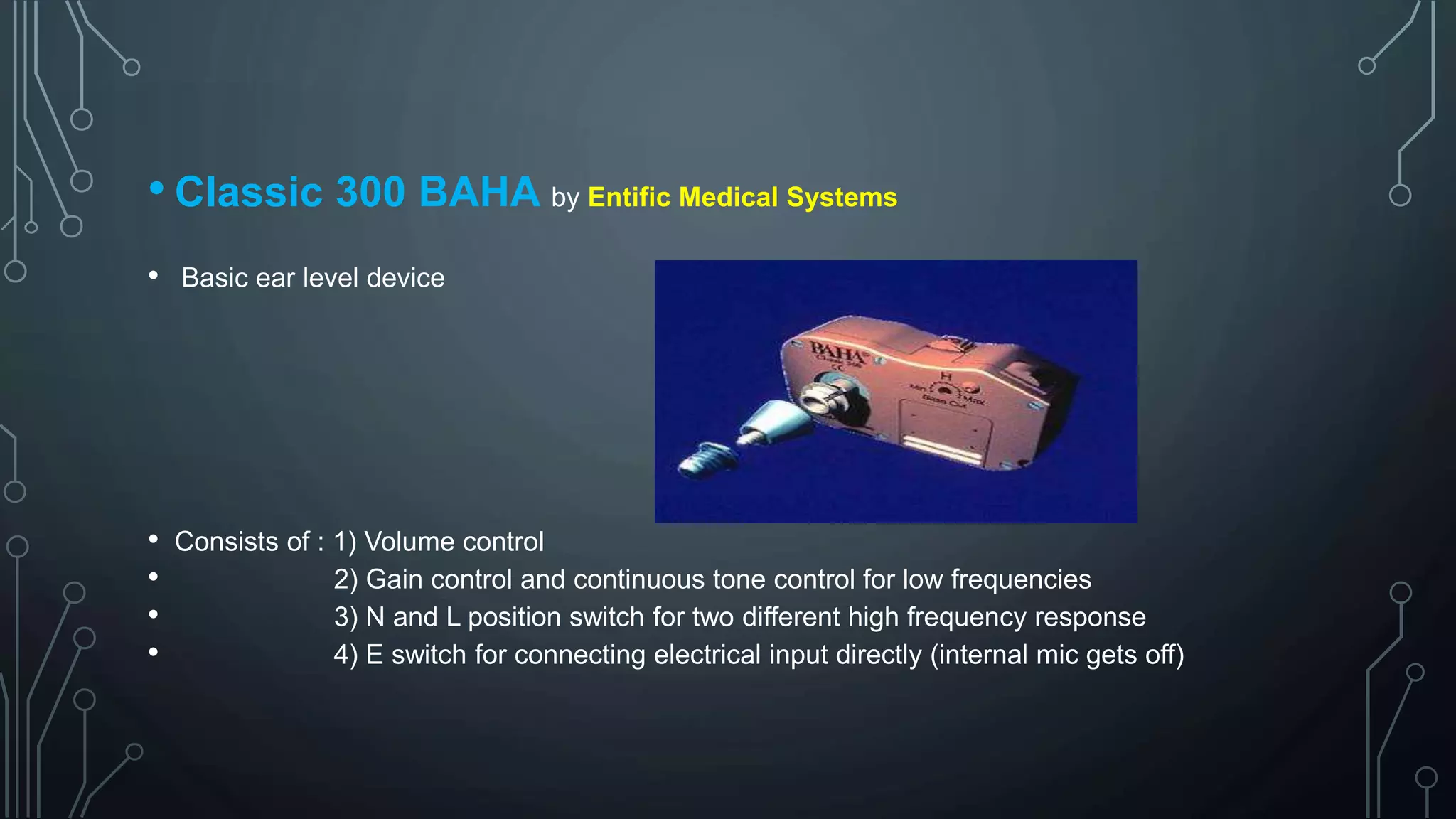
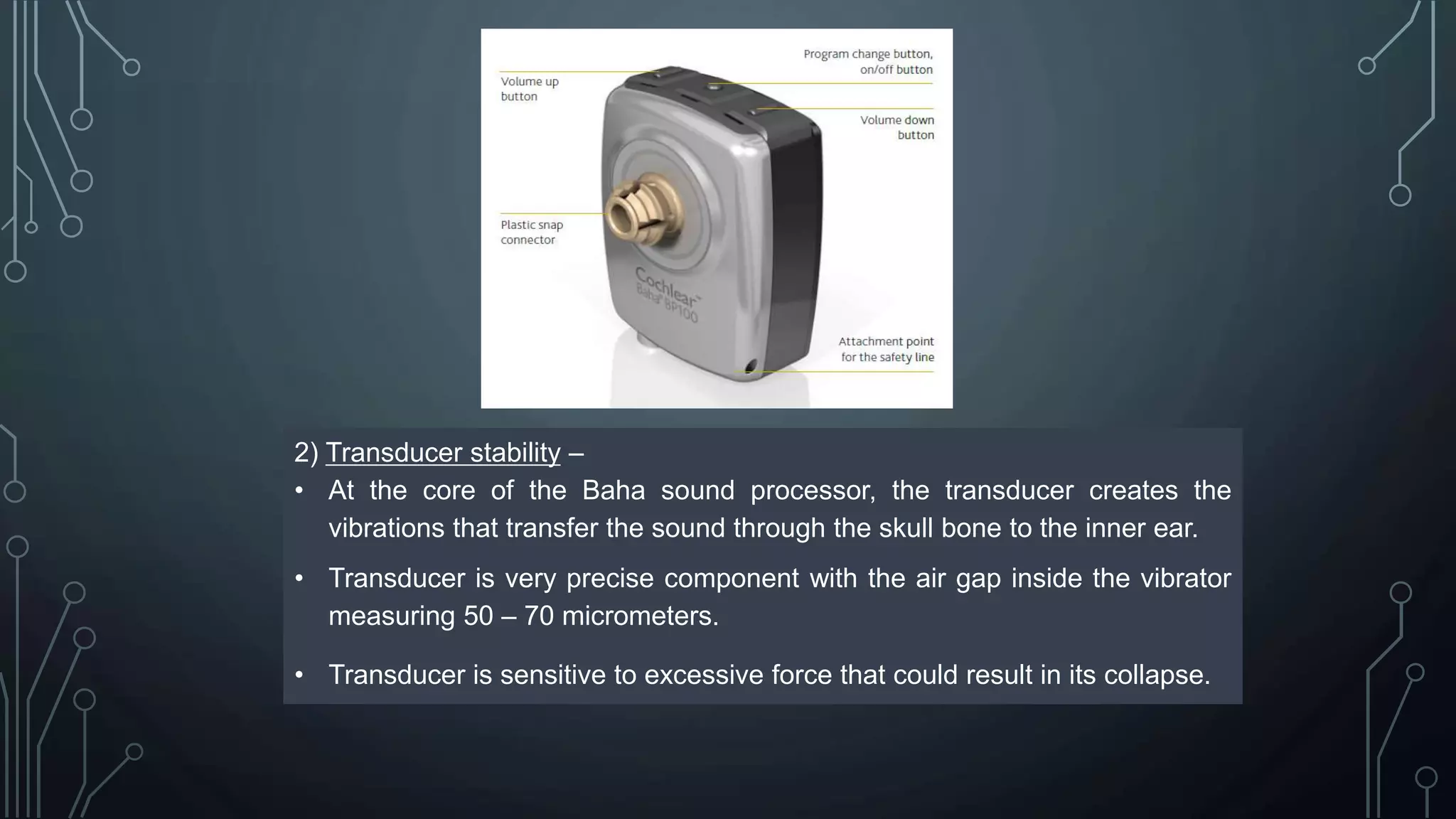
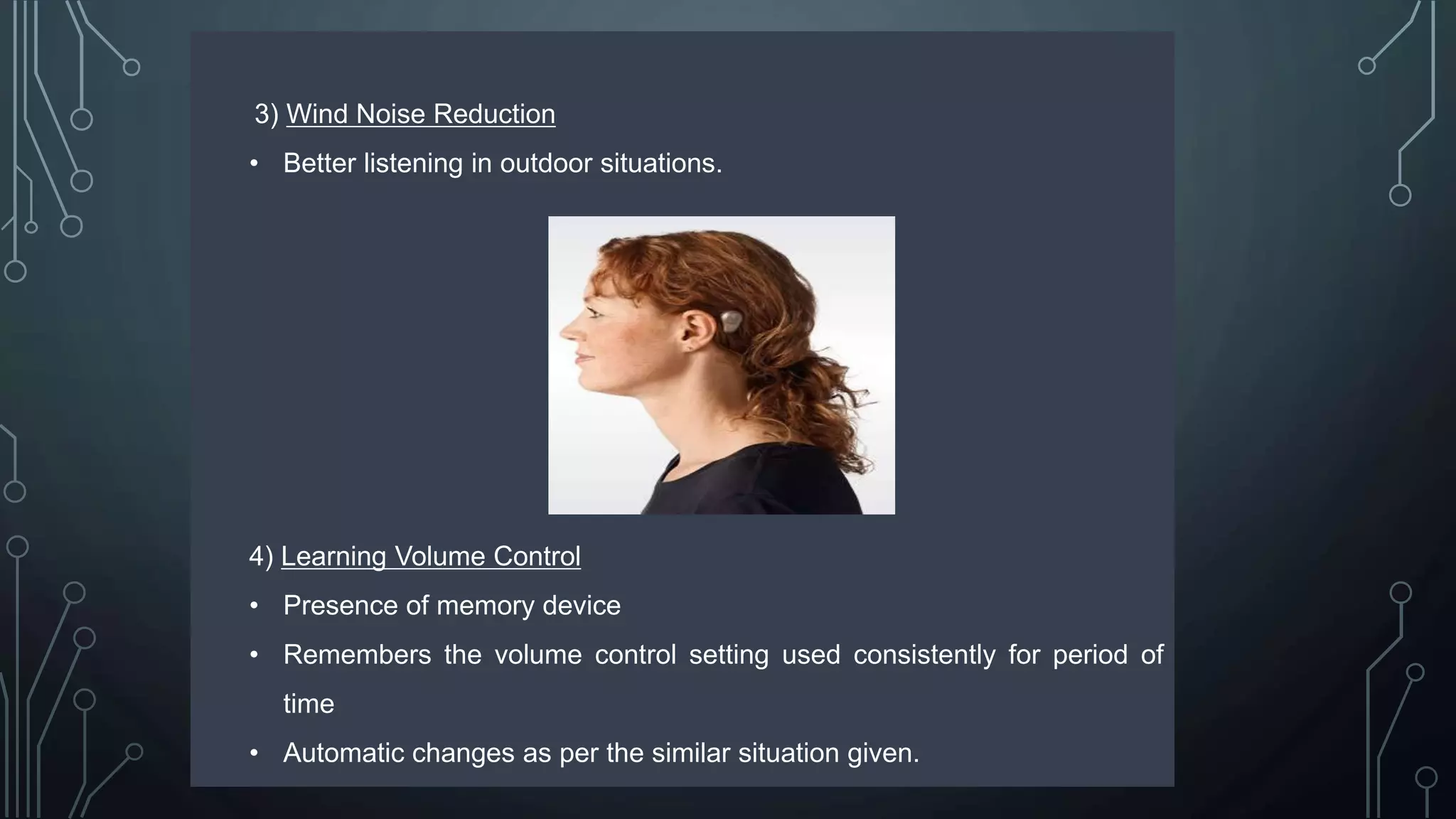
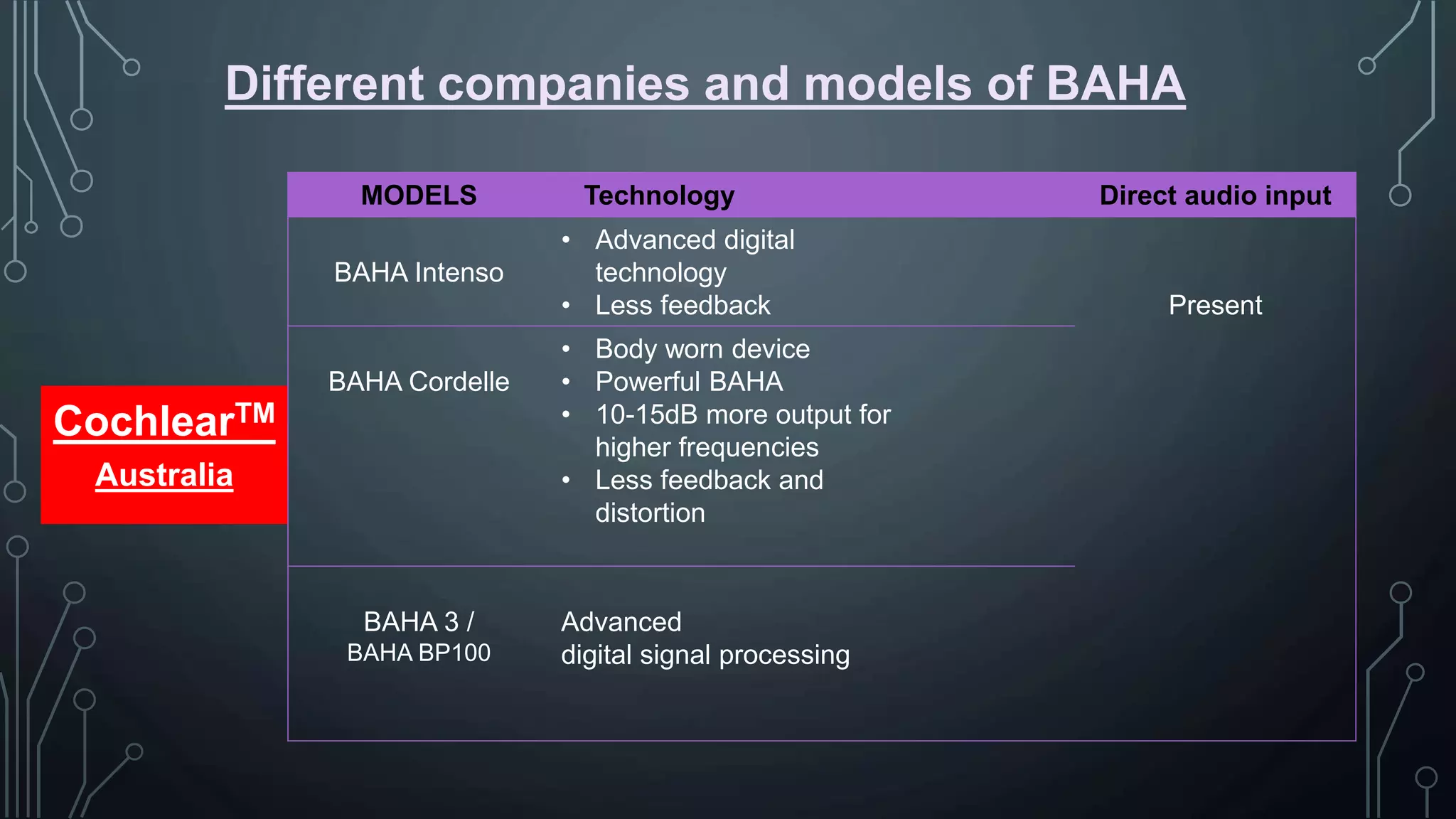
The document discusses the history, components, types, needs, candidacy, and surgery of bone anchored hearing aids (BAHA), which transmit sound to the cochlea via bone conduction by bypassing abnormalities of the outer and middle ear through an implanted titanium fixture. It traces the development of BAHA from its origins in the 1950s to current digital processors. BAHA consists of a titanium screw surgically implanted in the skull that protrudes a titanium abutment connecting to an external sound processor.