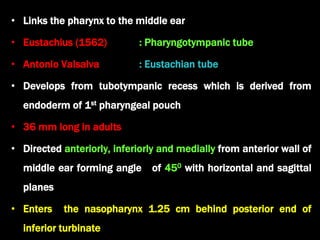
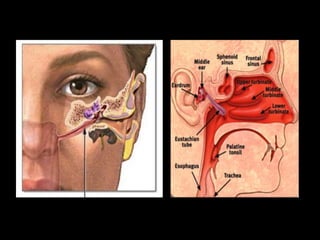
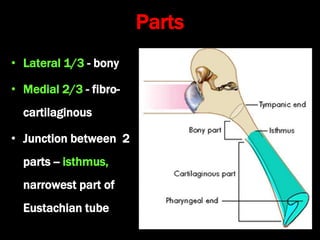
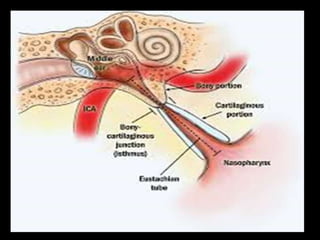
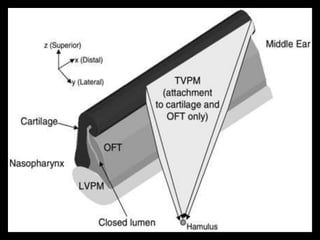
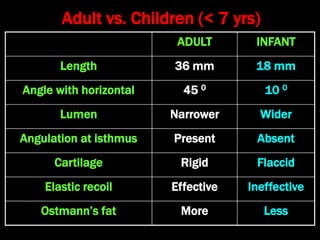
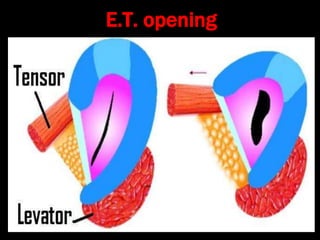
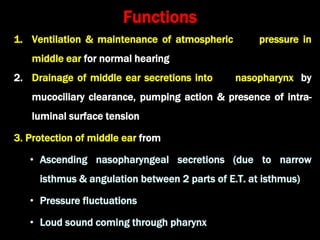
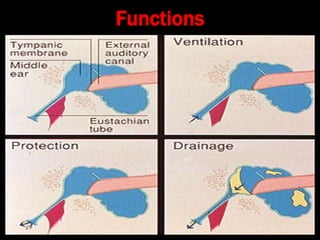
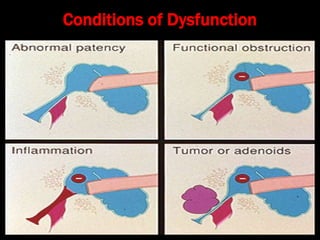
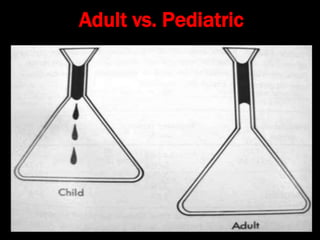
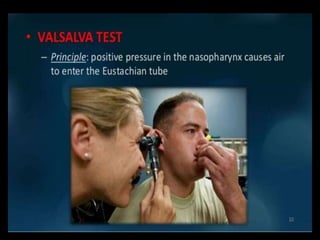
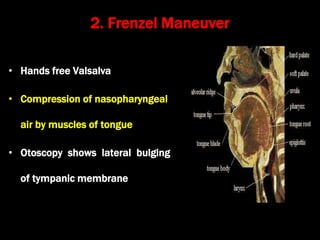
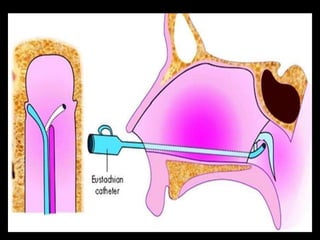
The Eustachian tube connects the middle ear to the nasopharynx. It is around 36mm long in adults and made of bone laterally and fibrocartilage medially. It opens with swallowing to equalize pressure and ventilate the middle ear. Dysfunction can cause ear infections and pressure issues. Evaluation involves tests like Valsalva, Toynbee maneuvers and tympanometry. Conditions like patulous Eustachian tube can also occur if it does not close properly.