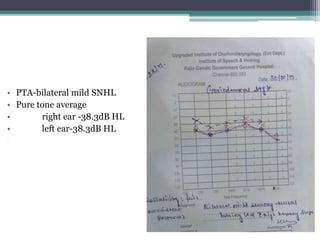
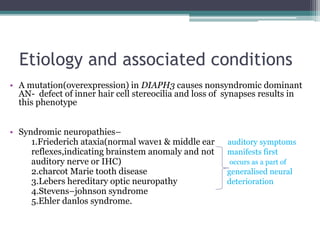
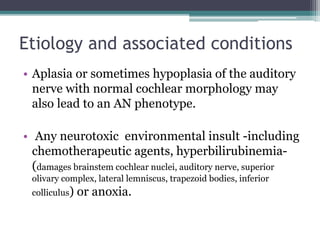
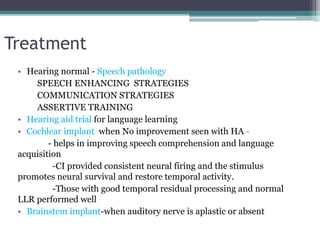
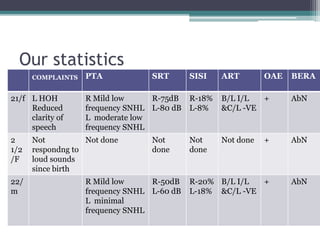
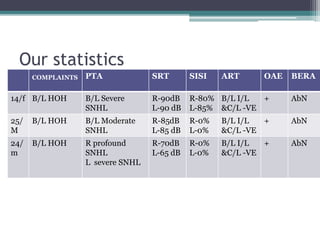
Auditory neuropathy spectrum disorder (ANSD) is characterized by normal outer hair cell function but abnormal or absent auditory brainstem response, despite mild to profound hearing loss. A 27-year-old female presented with right-sided hearing loss, vertigo, and tinnitus for several years. Testing found normal outer hair cell function but abnormal auditory brainstem responses, consistent with progressive ANSD. Treatment options for ANSD are limited but may include hearing aids, cochlear implants, or speech therapy depending on the severity and progression of the hearing loss.






















































![Polymer [ बहुलक ] Chemistry Notes PDF - Irfanullah Mehar - JJ Sir Chemistry.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/polymerchemistrynotespdf-irfanullahmehar-jjsirchemistry-260210172118-3f9b37f7-thumbnail.jpg?width=640&height=640&fit=bounds)













