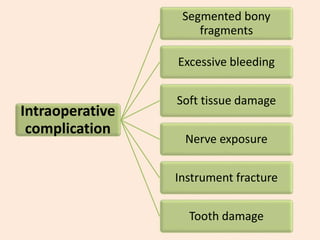
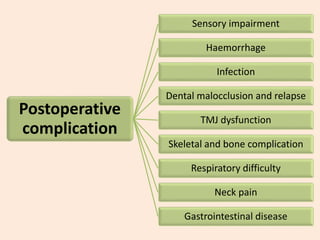
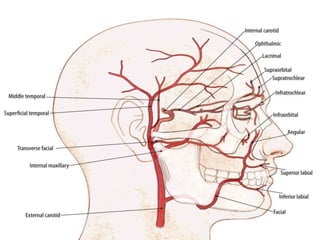
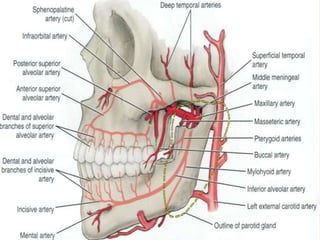
Common complications of orthognathic surgery include postoperative nausea and vomiting, infection, excessive bleeding, soft tissue damage, and nerve injuries. Intraoperative complications can include excessive bleeding, soft tissue damage, nerve exposure, and instrument fractures. Postoperative complications may involve sensory impairment, hemorrhage, infection, dental malocclusion, TMJ dysfunction, skeletal issues, and respiratory or neck pain. Soft tissue damage, hemorrhage, wound infection, nerve injuries, skeletal problems, and dental issues are some of the main risks involved.













































![Complications and management_slide[1] final to be put on slideshare](https://cdn.slidesharecdn.com/ss_thumbnails/complicationsandmanagementslide1finaltobeputonslideshare-130710114420-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)



































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)






