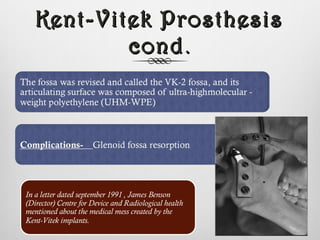
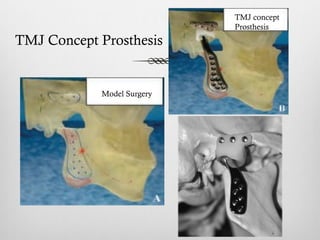
The document discusses reconstruction of the temporomandibular joint (TMJ) through various methods including autogenous grafts, alloplastic devices, distraction osteogenesis, and tissue engineering. Autogenous grafts that can be used include costochondral grafts, iliac crest grafts, fibular grafts, and coronoid process grafts, each with advantages and limitations. Alloplastic devices made of various materials are also discussed, including the Kent-Vitek prosthesis, Christensen's prosthesis, and TMJ Concepts prostheses. Distraction osteogenesis is described as a method to reconstruct the mandibular ramus through gradual distraction. Tissue engineering is mentioned as a potential future approach involving scaffolds























































































![TMJ ]Treatment options.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/tmjtreatmentoptions-230709162513-43034832-thumbnail.jpg?width=640&height=640&fit=bounds)


























