
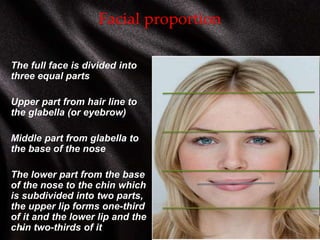

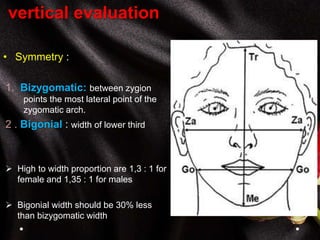
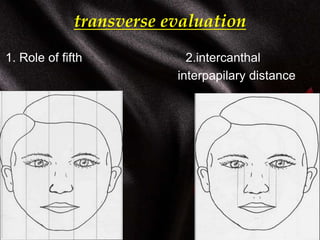
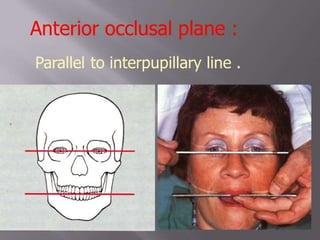

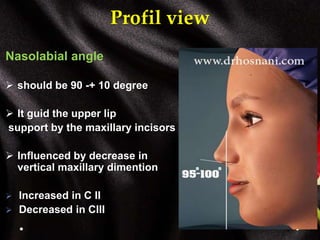
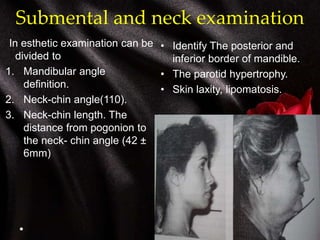
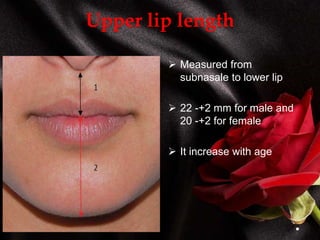
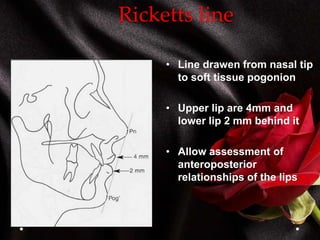

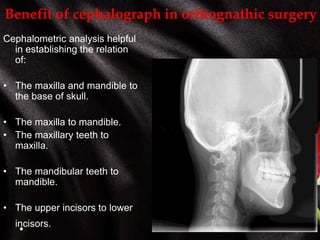
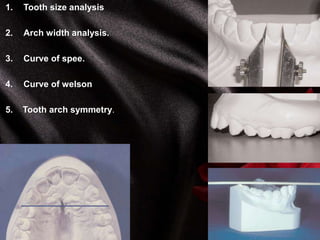
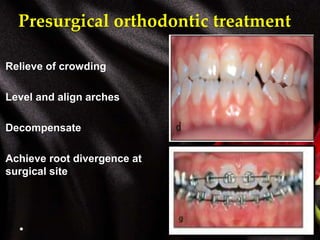
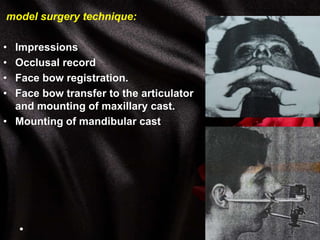
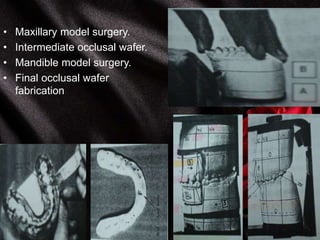

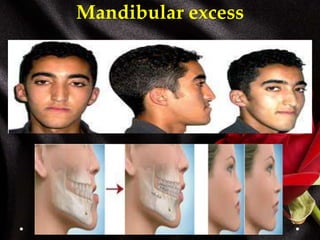

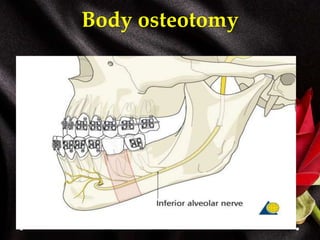
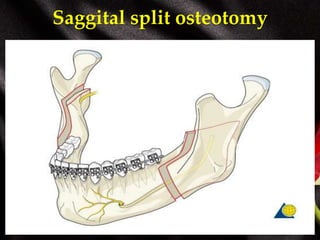
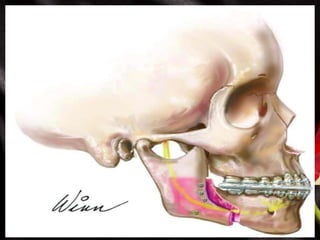
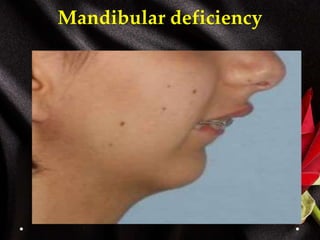

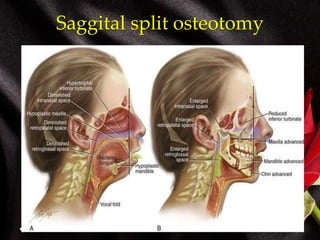
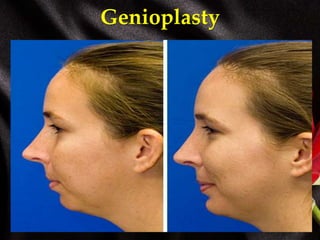
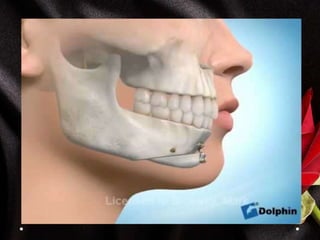
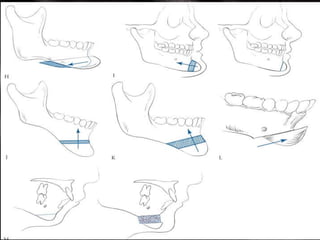

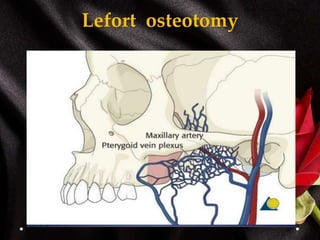
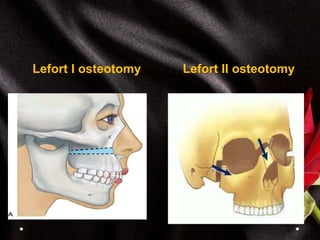
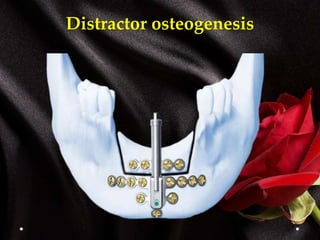




This document provides an overview of orthognathic surgery. It discusses the goals of orthognathic surgery which include obtaining normal function and facial harmony. It outlines the process of patient evaluation including history, examinations, investigations and treatment planning. Key parts of clinical evaluation such as frontal, vertical, transverse and profile assessments are described. The benefits of cephalometric analysis and dental model analysis are also summarized. Finally, it reviews various surgical techniques for treating mandibular and maxillary deficiencies and excesses, including osteotomies and distraction osteogenesis.






























































































