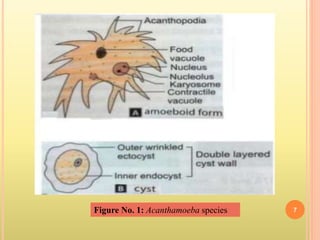
Acanthamoeba are free-living amoebae found worldwide in soil and water that can cause disease in humans. They have two life stages - a trophozoite stage and a cyst stage. They are known to cause Acanthamoeba keratitis through corneal trauma or contact lens use, as well as granulomatous amoebic encephalitis. Acanthamoeba keratitis is difficult to treat but can be managed with antimicrobial agents like propamidine isethionate and contact lens use should involve proper cleaning and disinfection to prevent infection.