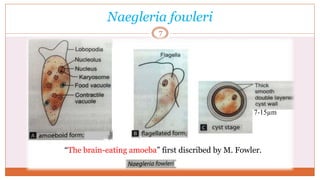
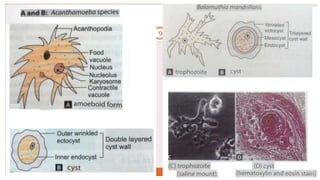
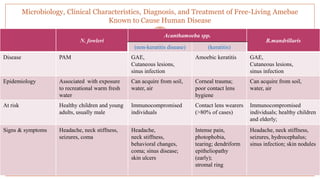
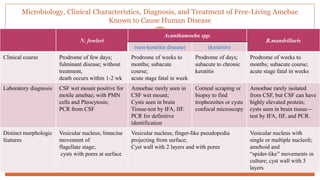
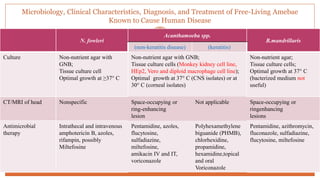
1. The document discusses various aspects of free-living amoebae (FLA) including Naegleria fowleri, Acanthamoeba spp., and Balamuthia mandrillaris.
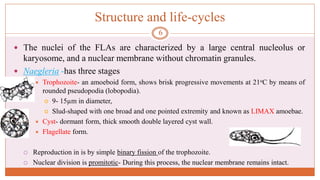
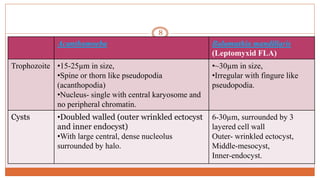
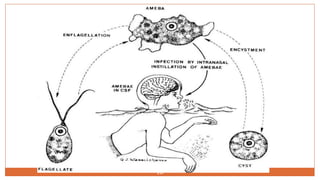
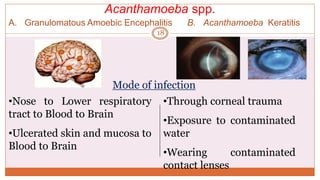
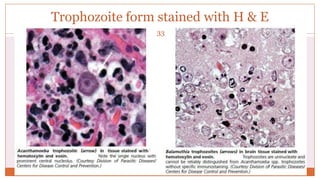
2. It covers their classification, structure, life cycles, modes of infection, clinical manifestations like primary amoebic meningoencephalitis and granulomatous amoebic encephalitis.
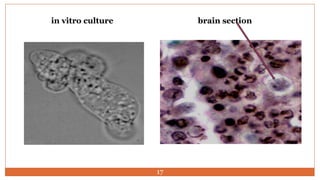
3. The summary also discusses their diagnosis through microscopy, culture, molecular and imaging techniques as well as challenges in treatment.