












![REFERENCES
• Contact Lens News and Information. (2012, February 20). Contact Lens Solutions Ineffective
Against Acanthamoeba, Study Finds. Retrieved August 10, 2012, from
http://t3.gstatic.com/images?q=tbn:ANd9GcTB4chV7tr0UeG44UKnU9qSBv4IOy_0_vA
JrnYHIvhM75iGwMF
• Centers for Disease Control and Prevention (CDC). Acanthamoeba - Granulomatous Amebic
Encephalitis (GAE); Keratitis. Retrieved August 11, 2012, from
http://www.cdc.gov/parasites/acanthamoeba/disease.html
• Centers for Disease Control and Prevention (CDC). Laboratory Identification of Parasites of
Public Health Concern; Free-Living Amebic Infections. Retrieved August 11, 2012, from
http://www.dpd.cdc.gov/dpdx/HTML/FreeLivingAmebic.htm
• Simon Kilvington, PhD. (2008). Physiological Response of Acanthamoeba to
Contact Lens Disinfectants [Powerpoint Format]. Retrieved August 11, 2012, from
http://www.google.com.ph/url?sa=t&rct=j&q=physiological%20response%20of%20ac
• Animal Planet. Monsters inside me. Acanthamoeba picture. Retrieved August 15, 2012,
from http://animal.discovery.com/invertebrates/monsters-inside-me/acanthamoeba-
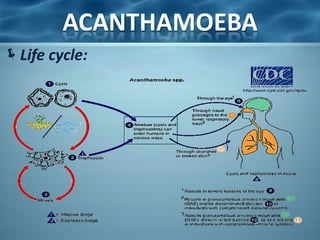
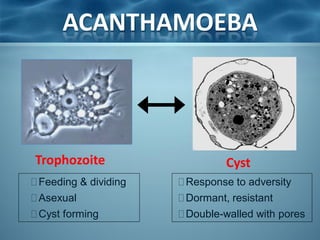
keratitis/](https://image.slidesharecdn.com/acanthamoeba-121125090945-phpapp02/85/Acanthamoeba-22-320.jpg)



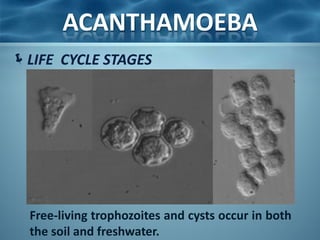
Acanthamoeba is a microscopic, free-living amoeba that can cause rare but severe infections of the eye, skin, and central nervous system. It has two stages in its life cycle - the trophozoite stage where it replicates and feeds, and the cyst stage where it becomes dormant and resistant. It is found in soil, water, and other environmental sources. When it enters the eye, it can cause Acanthamoeba keratitis, and when it enters the respiratory system or skin it can cause granulomatous amebic encephalitis by spreading to the brain. Treatment involves medications like pentamidine and antiseptic agents depending on the infected area.





















































