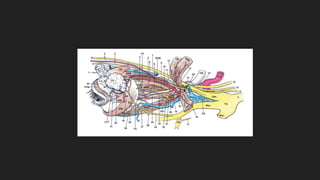
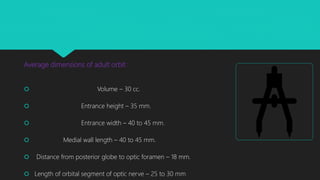
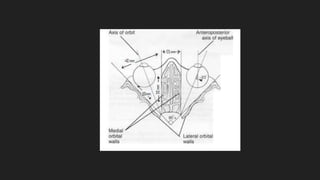
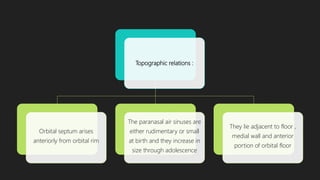
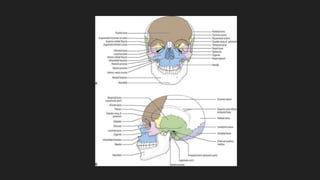
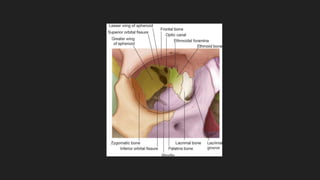
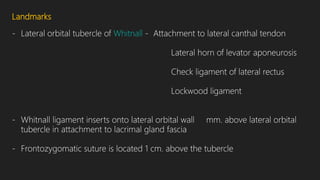
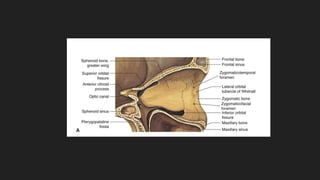
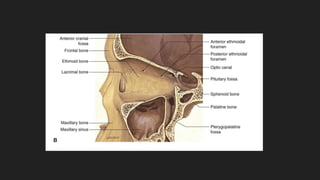
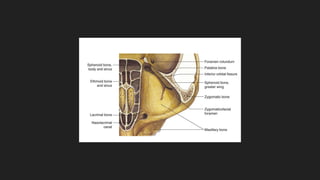
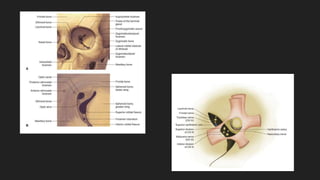
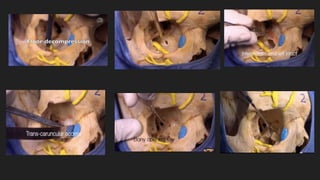
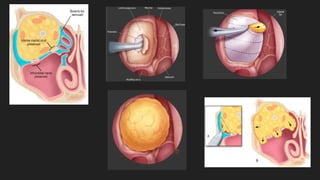
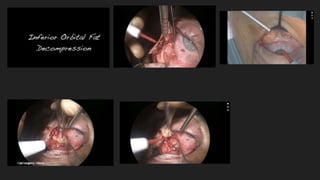
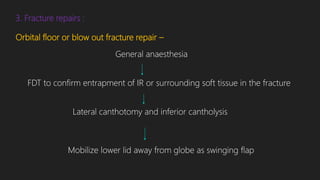
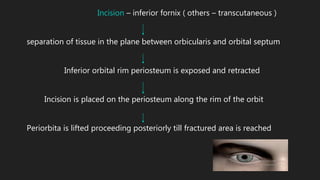
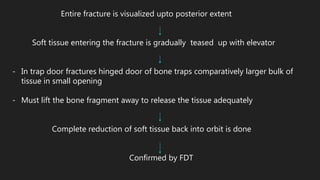
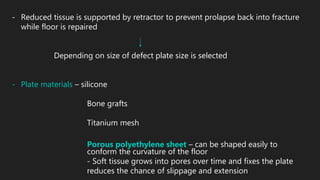
This document provides information on orbital surgeries and anatomy. It describes the average dimensions of the adult orbit and its topographic relations. The seven bones that make up the four orbital walls - roof, lateral wall, medial wall, and floor - are identified along with key landmarks. The document also discusses the five surgical spaces of the orbit and different surgical techniques for orbitotomy, orbital decompression, and fracture repair.