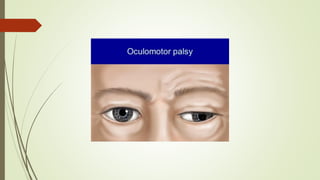
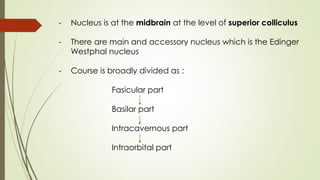
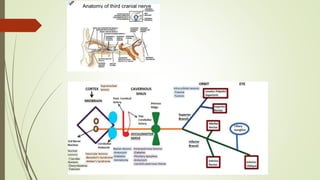
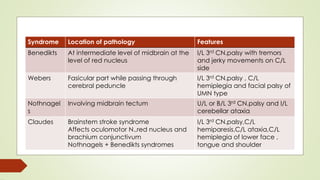
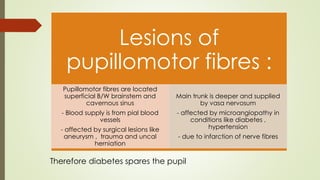
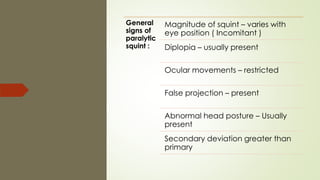
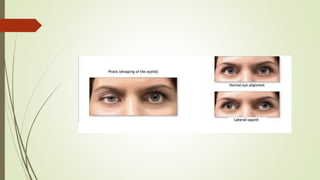
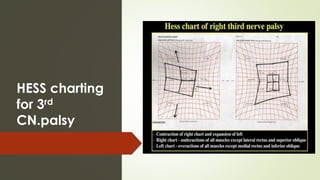
This document provides information about paralytic strabismus caused by a third cranial nerve palsy. It discusses the anatomy and supply of the oculomotor nerve. Signs of a third nerve palsy include ptosis, divergent squint with intorsion, restricted eye movements, and diplopia. Causes can include lesions of the nerve nuclei, nerve trunk, or intraorbital muscles. Investigation involves assessing eye alignment and movements to localize the site of lesion, with diplopia charting helping to differentiate nerve or muscle involvement.