Downloaded 111 times

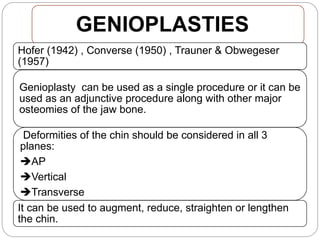
![MANDIBULAR OSTEOTOMIES
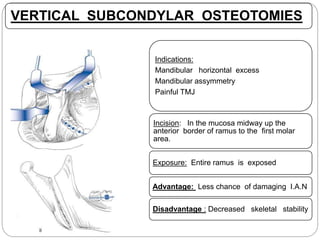
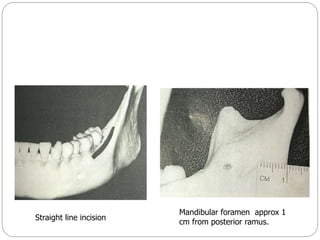
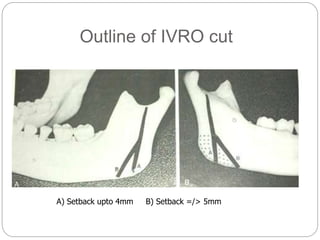
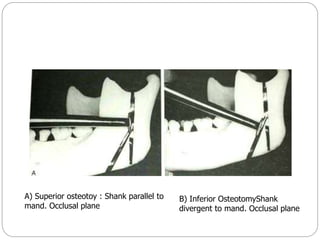
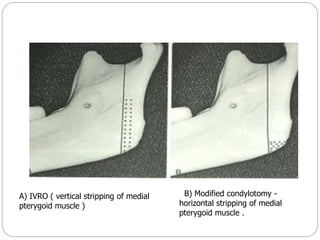
VERTICAL RAMUS OSTEOTOMIES
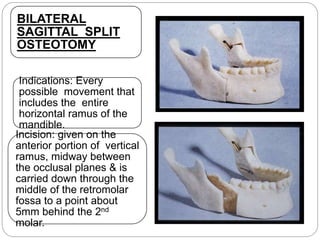
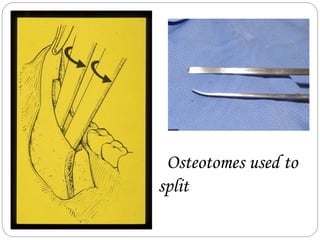
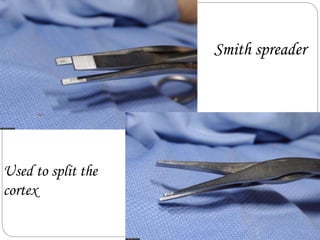
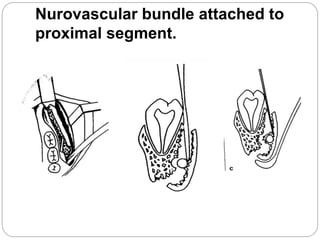
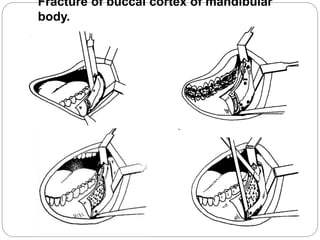
BILATERAL SAGITTAL SPLIT OSTEOTOMY
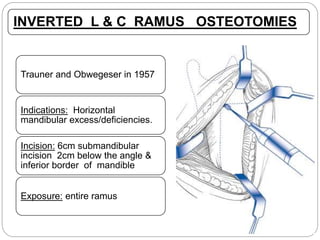
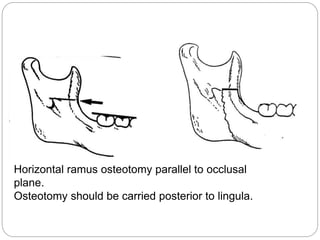
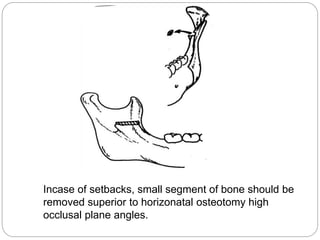
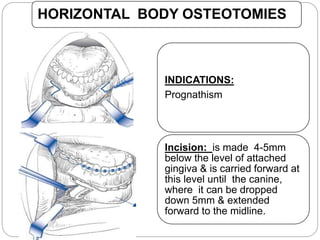
HORIZONTAL RAMUS OSTEOTOMIES
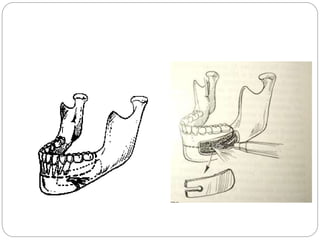
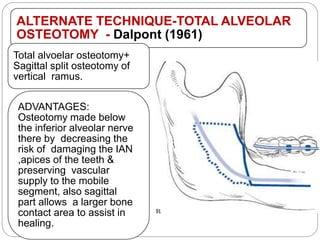
SUB APICAL OSTEOTOMIES [segmental osteotomies]
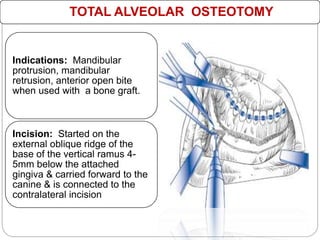
TOTAL ALVEOLAR OSTEOTOMIES
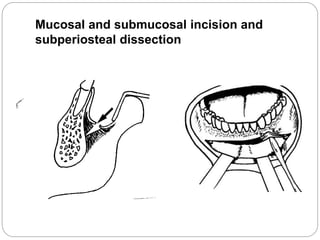
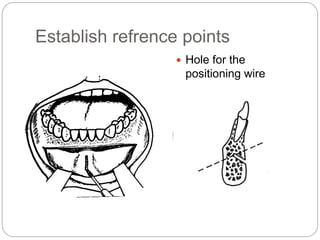
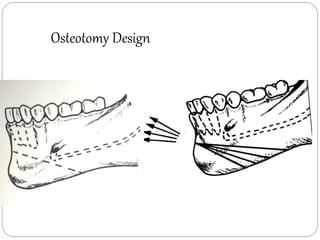
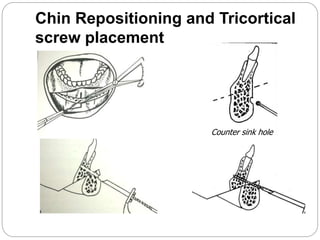
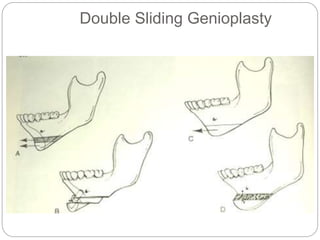
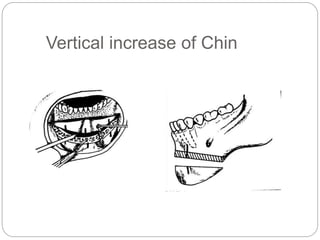
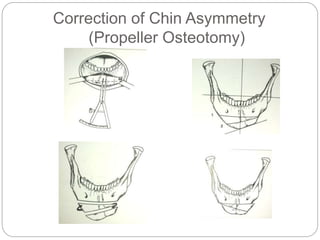
HORIZONTAL OSTEOTOMY OF SYMPHYSIS/ GENIOPLASTY](https://image.slidesharecdn.com/mandibularorthognathicproceduresi-ih-160522070242/85/Mandibular-orthognathic-procedures-1-ih-19-320.jpg)
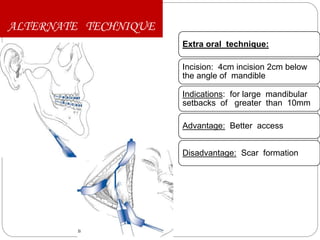
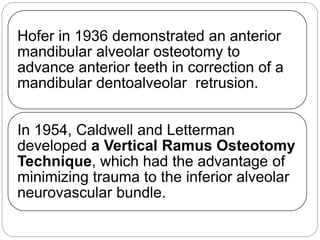
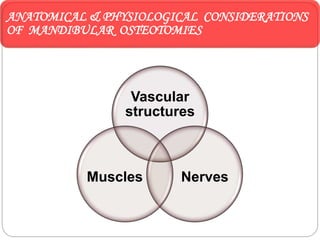
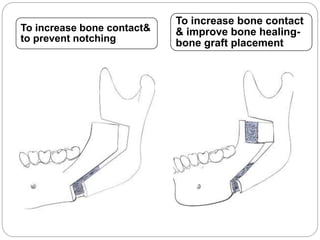
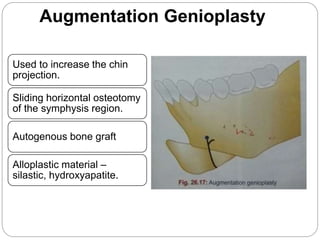
![ALTERNATE TECHNIQUES FOR
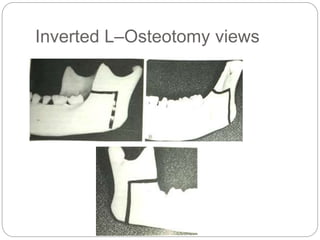
INVERTED L OSTEOTOMIES [C –
osteotomy]
Advantage :
To increase
the bone
contact
during
advancement](https://image.slidesharecdn.com/mandibularorthognathicproceduresi-ih-160522070242/85/Mandibular-orthognathic-procedures-1-ih-31-320.jpg)

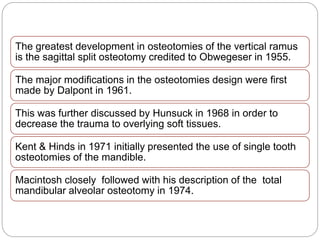
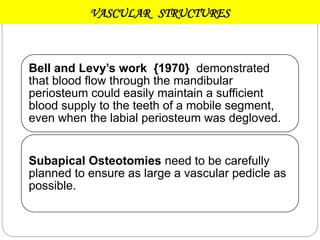
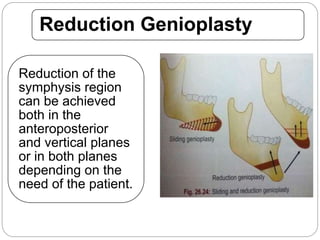
![ANTERIOR SUBAPICAL OSTEOTOMY
Indications: To move the anterior
mandible in every desirable
direction[ant,post,sup,inf-
repositioning]
Incision : is started 1cm behind
the planned vertical osteotomy&
is carried 4-5mm below the
attached gingiva & is brought to
the midline & connected with the
opposing incision.](https://image.slidesharecdn.com/mandibularorthognathicproceduresi-ih-160522070242/85/Mandibular-orthognathic-procedures-1-ih-59-320.jpg)
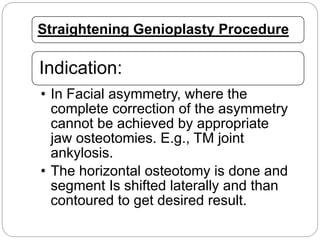
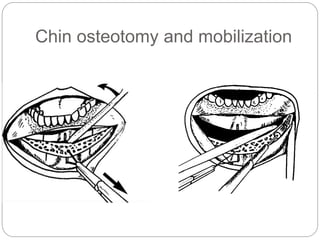

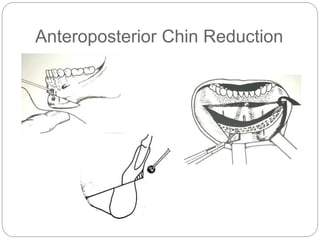
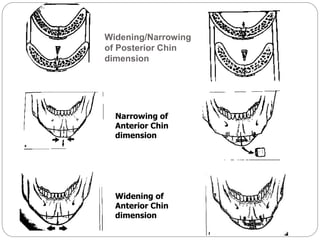
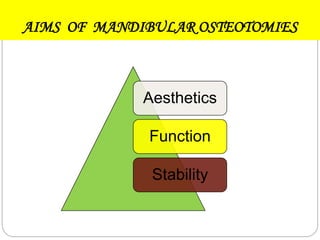
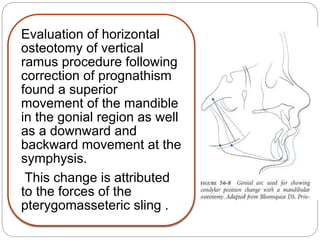
![dimensional reduction genioplasty. Keyhan
SO, Khiabani K, Hemmat S, Varedi P , Br J Oral
Maxillofac Surg.2013]](https://image.slidesharecdn.com/mandibularorthognathicproceduresi-ih-160522070242/85/Mandibular-orthognathic-procedures-1-ih-83-320.jpg)

This document provides an overview of mandibular orthognathic procedures. It begins with an introduction to orthognathic surgery and the history of mandibular osteotomies. It then discusses anatomical and physiological considerations, timing of osteotomies, and various osteotomy techniques including vertical ramus, sagittal split, horizontal ramus, subapical, and total alveolar osteotomies. It also briefly touches on soft tissue changes and complications that can occur with mandibular osteotomies. The document is intended as a reference for various mandibular orthognathic procedures.



































































